
Source: Rounding The Earth Author: Mathew Crawford
This past Saturday I had the honor of appearing with Nobel Peace Prize nominee Dr. Brian Tyson on Joe’s Place for a conversation about SARS-CoV-2, COVID-19, his results treating patients, and more. As far as these recorded discussions go, this was the most valuable of those I’ve had the opportunity to participate in.
It was good to see Brian on vacation—he has earned it. But how could one not be impressed by the giving nature of a man who would take two hours out of his poolside time to share his story?
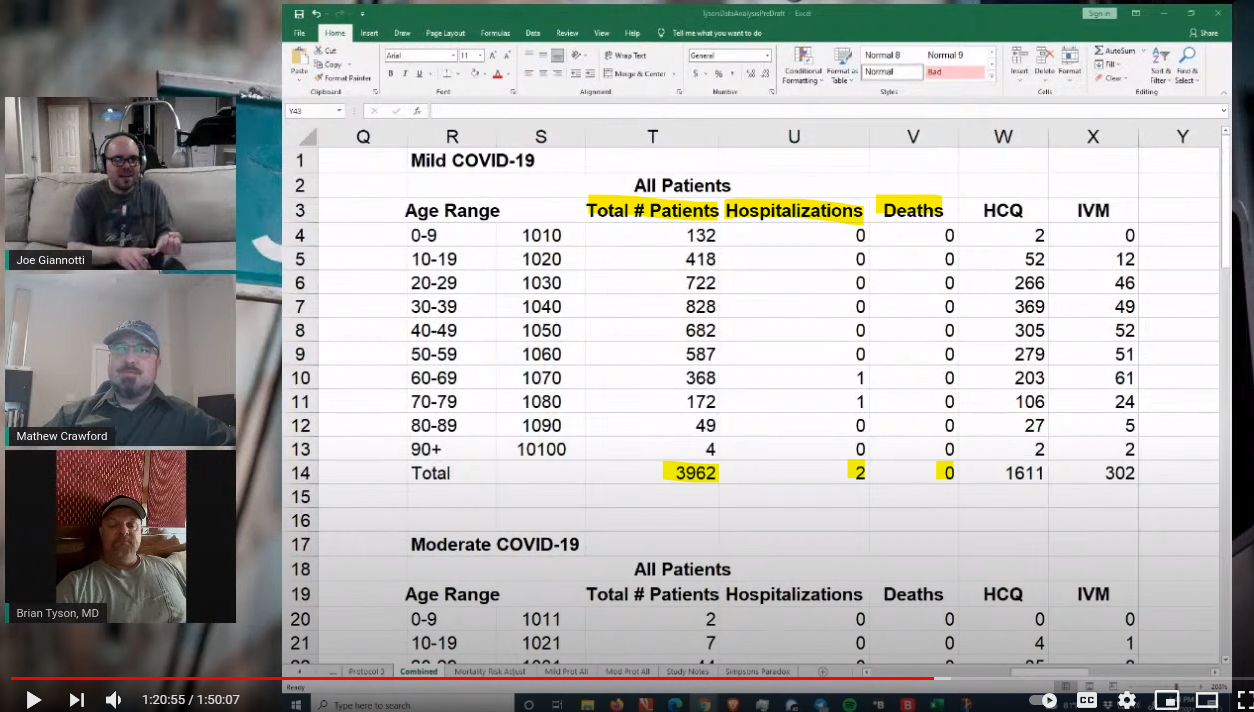
Early during the discussion, Brian shared the personal story of what motivated him to have his staff record the patient data for which he applied his protocol, based around hydroxychloroquine (HCQ) for those who needed it (ivermectin was later added), with a vitamin pack (including zinc) for all, macrolides where deemed appropriate, and sometimes steroids. Along with Dr. George Fareed, the pair have treated around 6,000 patients in Southern California, likely saving well over 100 lives in the process. They discuss their protocol here.
Brian previously sent me data from most of those patients, which I verified with Imperial County, cleaned (the data), and organized as a summary here. What is noteworthy is that of the 3962 patients who were treated early (prior to advancement to moderate COVID-19 as defined by the WHO), only 2 patients were hospitalized and 0 died. As I understand it, that total number of patients has grown to around 5,500 now, and as I found out Saturday, not one of their patients has returned to the clinics with long haul symptoms. These may be the best treatment results for any team anywhere in the world, and took place in one of the U.S. counties with the highest mortality rate per case.
Brian and George have been honored as nominees for the Nobel Peace Prize, along with other doctors who have stood fast against a tide of pressure, a top-down medical establishment that pretends their results are not meaningful, stark silence or dismissal in the legacy media reporting, and even death threats. Brian is quick to pass credit to those who began paving the road he took, citing Professor Didier Raoult and Dr. Vladimir Zelenko for bringing attention to HCQ as an effective treatment for COVID-19.
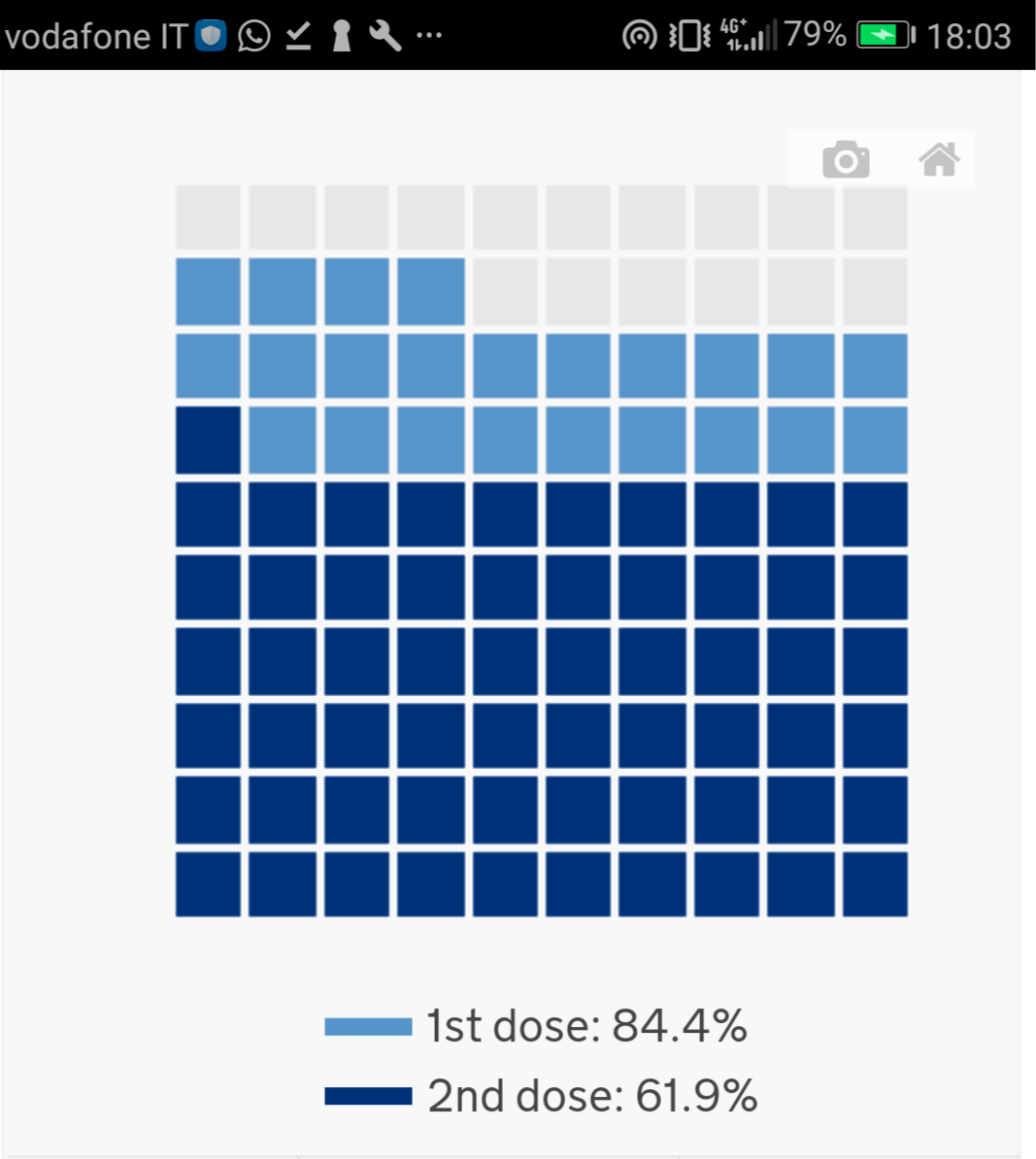
One important piece of the conversation we had involved what we’ve learned from the Public Health of England data (here, here, and here). I previously noted the oddity that while the vaccines used in the UK (primarily mRNA) do show efficacy in preventing COVID-19 symptoms (in the ballpark of 35% for one dose, and 80% for two doses), my analysis of the data seemed to indicate an efficacy of around 60% in preventing mortality. But here is the weirdest part: I calculated the mortality efficacy of the first dose to be better than the mortality efficacy from being fully vaccinated! And I’m not the only person to make that observation. These numbers are higher than the ones I computed after the June 25 PHE report, but are quite odd.
While thinking through what could account for the decline in mortality protection from the second dose, I imagined how the ledger of results might be broken down, along with my proposed redefinition of COVID. While adverse events reports have not been well analyzed as of yet (the precautionary principle puts that onus on those pushing new vaccines!), it seems likely that there are at least some excess deaths due to the vaccines. Suppose that getting a second dose does not reduce efficacy in preventing COVID-19 mortality, then it must be the case that those who died from the second dose were among those who would have died from a COVID-19 infection. This makes sense if there is some small part of the population which is unhealthy or genetically predisposed to producing enough spiked protein that the body cannot handle it. Regardless of what studies of size N = 14 say about the amount of observed spike protein circulating in a few patients, we are looking for events as rare as perhaps 1 in 10,000 or 1 in 100,000.
Once we realize that deaths due to vaccines overlap highly with deaths due to COVID-19 in the patient pool, we must accept the following:
- The data from the vaccine trials must be recalculated under the lens that some of the serious adverse events (SAEs) should be treated as COVID-19 cases.
- There may not be any vaccine efficacy in the data at all if some of the post-vaccination deaths are due to vaccine-induced COVID-19. It could even be the case that the mortality efficacy goes negative. My implied lives saved calculations put this easily in the realm of possibility. The only way to know is for authorities to organize and compile the data. And while a risk analysis is certainly due after more than six months of hundreds of millions of doses delivered, there is little indication authorities have bothered with the process. That’s more than a bit unsettling.
Of course, this is one of the several reasons why the raw data should be made available.
The Chloroquine Wars Part XX – Why The Early Treatment Data is Better Than Anyone Imagines
Dr. Peter McCullough’s Common Sense Breakdown of the Pandemic – The Chloroquine Wars Part XXIII
Doctor Didier Raoult Part I: Where We Are Now -The Chloroquine Wars Part XXV
What if the SARS-CoV-2 Virus is Weaker Than Most Everyone Thinks? – The Chloroquine Wars Part XXVIII
How to Rig Research: The WHO Edition – The Chloroquine Wars Part XXXIII
How to Rig Research: The WHO Edition Part II – The Chloroquine Wars Part XXXIV
The Meta-Analytical Fixers: An Ivermectin Tale – The Chloroquine Wars Part XL