

Source: Science Direct
Abstract
Background
The COVID-19 outbreak challenges the Spanish health system since March 2020. Some available therapies (antimalarials, antivirals, biological agents) were grounded on clinical case observations or basic science data. The aim of this study is to describe the characteristics and impact of different therapies on clinical outcomes in a cohort of severe COVID-19 patients.
Methods
In this retrospective, single-center, observational study, we collected sequential data on adult patients admitted to Hospital Universitario Quironsalud Madrid. Eligible patients should have a microbiological (positive test on RT-PCR assay from a nasal swab) or an epidemiological diagnosis of severe COVID-19. Demographic, baseline comorbidities, laboratory data, clinical outcomes, and treatments were compared between survivors and non-survivors. We carried out univariate and multivariate logistic regression models to assess potential risk factors for in-hospital mortality.
Findings
From March 10th to April 15th, 2020, 607 patients were included. Median age was 69 years [interquartile range, {IQR} 22; 65% male). The most common comorbidities were hypertension (276 [46·94%]), diabetes (95 [16·16%]), chronic cardiac (133 [22·62%]) and respiratory (114 [19·39%]) diseases. 141 patients (23·2%) died. In the multivariate model the risk of death increased with older age (odds ratio, for every year of age, 1·15, [95% CI 1·11 – 1·2]), tocilizumab therapy (2·4, [1·13 – 5·11]), C-reactive protein at admission (1·07, per 10 mg/L, [1·04 – 1·10]), d-dimer > 2·5 μg/mL (1·99, [1·03 – 3·86]), diabetes mellitus (2·61, [1·19 – 5·73]), and the PaO2/FiO2 at admission (0·99, per every 1 mmHg, [0·98 – 0·99]). Among the prescribed therapies (tocilizumab, glucocorticoids, lopinavir/ritonavir, hydroxychloroquine, cyclosporine), only cyclosporine was associated with a significant decrease in mortality (0·24, [0·12 – 0·46]; p<0·001).
Interpretation
In a real-clinical setting, inhibition of the calcineurin inflammatory pathway, NF-κΒ, could reduce the hyperinflammatory phase in COVID-19. Our findings might entail relevant implications for the therapy of this disease and could boost the design of new clinical trials among subjects affected by severe COVID-19.
Funding
Hospital Universitario Quironsalud Madrid. Own fundings for COVID-19 research.
Keywords
Severe COVID-19SARS-CoV-2 infectionCyclosporine aAcute respiratory insufficiencyImmunosuppressantsHyperinflammation state
1. Introduction
Research in context
Evidence before this study
We searched PubMed, up to March 12, 2020, for published clinical studies describing therapies in different cohorts of hospitalized COVID-19 patients. The search terms were “COVID-19″, “SARS-CoV-2″, and “therapy”.
Severe COVID-19 occurs more frequently in people harboring chronic diseases – about all those with cardiovascular or chronic lung conditions, obesity, and diabetes mellitus. Contrary to the first expectations, immunosuppressed patients were infrequent reported in large clinical cohorts of COVID-19. Therefore, in-hospital mortality could be more influenced by these previous risk factors than by the immunosuppression itself.
We found that there were no approved therapies for this condition. Some of the described empiric approaches included antiviral compounds or immunomodulatory drugs. The efficacy of all of them was not defined yet.
Added value of this study
In a real-clinical setting, inhibition of the calcineurin inflammatory pathway, NF-κB, using cyclosporine A (CsA) showed a reduction in the odds ratio for death in hospitalized patients affected by severe COVID-19 (odds ratio (0·24, [0·12 – 0·46]); p<0·001. This finding was observed in a population of patients who had baseline comorbidities and risk factors for in-hospital death similar to former research of the same scope. In this way, we hypothesize that CsA could block the hyperinflammatory phase in COVID-19.
Implications of all the available evidence
Here, we report one of the first clinical reports of the positive effect of CsA on in-hospital mortality associated with severe COVID-19, used as a first-line drug. These results, based on a retrospective analysis of observational data in single-center, should encourage the development of a randomized, multicenter, clinical trial to assess the efficacy and safety of CsA in the treatment of patients with severe COVID-19.
The outbreak of the disease caused by SARS-CoV-2 has become a global health problem since its first-time description in December 2019 in Wuhan, China [1]. This novel virus belongs to the same coronaviruses (CoVs) family such as SARS-CoV and MERS-CoV [2]. All can cause rapid and severe acute respiratory distress [3]. So, the health systems of several countries are facing an unprecedented challenge. Until the first pandemic wave, there has not been any proven efficacious drug against SARS-CoV-2. In this context, the therapeutic protocols focus on supportive measures. Furthermore, some therapies against SARS-CoV-2 are grounded in clinical case series and basic science research.
The coronavirus disease 2019 (COVID-19) in hospitalized patients has a high case-mortality rate [4,5] with deaths caused by respiratory failure, and many patients might need mechanical ventilation [6]. Some drugs have been available, including antimalarials [7,8], antivirals [9], or monoclonal antibodies – such as tocilizumab, an antibody against the soluble receptor of interleukin-6 (IL-6) [10,11]. Regardless, their true impact on the course of the disease was unknown at the beginning of the pandemic. In these circumstances, urgent needs arise to know the results of different treatments and approaches. Thereby, they could help to guide the design of randomized clinical trials (RCTs).
The spread of severe SARS-CoV-2 infection has been, unfortunately, quick. The selection and development of RCTs might take a long time – if scientific and ethical standards are to be met. Most of the first patients with severe COVID-19 were not a candidate to RCTs, due to the strict inclusion criteria. Last, limitations of the use of some drugs imposed by the local health authorities [12] and stock shortages become a recent concern.
Two central processes occur in SARS-CoV-2 infection. At first, viral replication predominates. Then, during the second week, a hyperinflammation state becomes progressively stronger [13]. This hyperimmune response leads to the development of a cytokine storm syndrome and, hence, acute pulmonary injury [14,15,16].
The SARS-CoV-2 virion hijacks the human angiotensin-converting enzyme 2 (ACE2) receptor for cell entry [17]. CoVs replication relies on several host factors, but mainly cyclophilin A (CypA) [18]. This peptidyl-propyl isomerase, CypA, plays an important role in the signaling and activation of the nuclear factor binding near the κ-light chain gene in B cells (NF-κB) – and also in the regulation of the nuclear factor of activated T cells’ (NFAT) inflammatory pathway. Both are key components of the immune response and, hence, of the cytokine release storm [19]. Cyclosporine A (CsA) is a well-known immunosuppressant drug, whose action depends on interaction with intracellular Cyps [16,20]. Cell cultures’ experiments proved that CsA might inhibit the replication of CoVs. Hence it would modulate and control the deleterious immunopathogenic response [18,21]. Thus, we decided to include CsA as an off-label (or compassionate) drug in our COVID-19 protocol.
The current research aims to describe the clinical characteristics and impact of different therapies on clinical outcomes of patients with severe COVID-19 hospitalized in our center.
2. Methods
2.1. Study design and participants
We designed a retrospective, observational, longitudinal study at Hospital Universitario Quironsalud Madrid, sited in Pozuelo de Alarcon, Madrid, Spain. It is a tertiary care, academic medical center, serving approximately 2,500,000 citizens – those with health insurance care provided by various private companies, and public workers who are mutual society members, or its beneficiaries, in the Community of Madrid. Furthermore, during the COVID-19 pandemic, we admitted any required transfers from the National Health System in the Madrid Region.
The Research Ethics Committee of the Fundación Jiménez Diaz (code EO0083–20 HUQM) approved the study protocol. We obtained a signed written consent form from all patients (oral consent, or from a patient’s legal representative, was also admitted – as some patients were too unwell to provide written consent).
Patients included in the study were those admitted to the hospital between March 10th and April 15th, 2020, and then followed up until May 12th, 2020, the day of the last recorded event (in-hospital death or alive/discharge).
To define a COVID-19 pneumonia case, we followed two sets of criteria. First, clinical criteria: eligible cases must have pneumonia confirmed by chest imaging (computer tomography or radiography [22,23]) and oxygen saturation (SaO2) at or below 94% while breathing ambient air, or a ratio of the partial pressure of oxygen (PaO2) to a fraction of inspired oxygen (FiO2) (PaO2/FiO2; or PAFI) at or below 300 mmHg. When PaO2 was not available, a pulse oximetric saturation (SaO2) to FiO2 ratio (SaO2/FiO2; or SAFI) was recorded – considering the next equivalence: SAFI of 235 and 315 mmHg would correlate to PAFI of 200 and 300 mmHg, respectively [24]. Second, microbiological criteria. Those cases were eligible under three circumstances. One, if they had any positive result on polymerase chain reaction (PCR) testing of a nasopharyngeal swab against SARS-CoV-2 during admission. Two, after an initial negative PCR result, but a typical clinical scenario of SARS-CoV-2 infection. And three, a distinguished clinical picture even without conducting a PCR assay, according to local epidemiology [25].
2.2. Outcomes
The primary end-point was in-hospital mortality. The secondary outcomes were the total length of stay, the number of patients admitted to the intensive care unit (ICU), length of stay in the ICU, percentage who required mechanical ventilation, or non-invasive ventilation.
2.3. Data collection
We collected data using the electronic health records, from the time of admission to completion of the care episode. These data included demographic information, baseline comorbidities, radiographic and laboratory tests, inpatient medications against COVID-19, and outcomes. We compared the laboratory results obtained in the first 24 h of admission with the last ones available before the outcome.
Exclusion criteria included pregnancy or breast-feeding, age under 18 years old, known allergy or hypersensitivity to any drug included in the protocol, advanced dementia, vital prognosis less than 6 months according to best physician judgment, chronic renal insufficiency with a filtration rate under 25 ml/min/1·73m2, untreated hepatitis B or C infection, known severe liver disease (transaminase levels more than 5 times the upper limit of the normal range or hepatic cirrhosis class Child-Pugh B or C), previous uncontrolled arterial hypertension, prolonged QTc interval at triage, or any concomitant medication that contraindicated any of the selected drugs in the protocol. We also excluded those patients who were only under supportive care owing to their severe condition, which precluded any benefit from active treatments, and hence, with a high probability of death in the next 24 h after admission, according to criteria of the attending team, precluded any benefit from active treatments.
2.4. Treatments
Table 1S contains a summary of our protocol. Below, we include some comments to explain the use of CsA.
Table 1. Baseline characteristics of patients hospitalized with COVID-19 according to survival outcome.
| Characteristics | All patients | Survivors | Non-survivors | P value* | |||
|---|---|---|---|---|---|---|---|
| (n = 607) | (n = 466, 76·8%) | (n = 141, 23·2%) | |||||
| Age, yrs -Median (IQR) | 69·00 | [22.00] | 65·00 | [21·00] | 79·00 | [12·00] | <0·001 |
| Sex (n,%) | |||||||
| Female | 212 | 34·98% | 296 | 63·66% | 98 | 69·50% | 0·202 |
| Male | 394 | 65·02% | 169 | 36·34% | 43 | 30·50% | |
| Chest X-ray score -Median [IQR] | 6·00 | [3·00] | 5·00 | [2·00] | 6·00 | [2·00] | <0·001 |
| Non-invasive mechanical ventilation/Boussignac (Yes; n,%) | 30 | 4·94% | 25 | 5·36% | 5 | 3·55% | 0·383 |
| Invasive mechanical ventilation (Yes; n,%) | 45 | 7·41% | 21 | 4·51% | 24 | 17·02% | <0·001 |
| Days on mechanical ventilation – Median [IQR]. | 11·00 | [16·00] | 10·00 | [16·00] | 11·00 | [15·50] | 0·459 |
| Intensive care unit (ICU) admission (Yes; n,%) | 49 | 8·07% | 25 | 5·36% | 24 | 17·02% | <0·001 |
| Length of stay, ICU – Median [IQR], d. | 11·00 | [13·50] | 11·00 | [17·00] | 11·00 | [13·75] | 0·120 |
| Length of stay (total) – Median [IQR], d. | 8.00 | [9·00] | 8·00 | [9·00] | 6·00 | [6·00] | 0·001 |
| Absolute white-cell count at admission; × 10−9/liter -Median [IQR] | 6·88 | [4·24] | 6·62 | [3·88] | 8·08 | [5·19] | <0·001 |
| Lymphocyte count at admission; × 10−9/liter -Median [IQR] | 0·90 | [0·60] | 1·00 | [0·70] | 0·80 | [0·60] | 0·003 |
| Lymphocyte count at nadir; × 10−9/liter -Median [IQR] | 0·70 | [0·50] | 0·80 | [0·50] | 0·60 | [0.40] | <0·001 |
| Lymphocyte count at outcome; × 10−9/liter -Median [IQR] | 1·30 | [1·00] | 1·50 | [0·80] | 0·70 | [0·50] | <0·001 |
| Ferritin at admission; μg/liter – Median [IQR] | 1067·50 | [1380·25] | 925·00 | [1344·00] | 1371·00 | [2097·00] | 0·001 |
| Ferritin at admission | |||||||
| ≤ 1000, μg/liter | 210 | 49·30% | 175 | 51·62% | 35 | 40·23% | 0·058 |
| > 1000, μg/liter | 216 | 50·70% | 164 | 48·38% | 52 | 59·77% | |
| Ferritin at outcome; μg/liter – Median [IQR] | 801·50 | [990·25] | 722·00 | [827·00] | 1464·00 | [2566·00] | <0·001 |
| C-reactive protein at admission; mg/liter (upper limit 5) -Median [IQR] | 130·73 | [170·74] | 120·02 | [150·34] | 220·32 | [200·38] | <0·001 |
| C-reactive protein at outcome; mg/liter (upper limit 5) -Median [IQR] | 10·96 | [70·23] | 10·28 | [30·58] | 120·76 | [200·52] | <0·001 |
| Aspartate aminotransferase; U/L (upper limit 34)- Median [IQR] | 48·00 | [56·00] | 46·00 | [50·00] | 66·80 | [82·08] | <0·001 |
| Alanine aminotransferase; U/L (upper limit 49)- Median (IQR) | 50·00 | [68·50] | 52·00 | [67·75] | 42·00 | [65·50] | 0·026 |
| Lactate dehydrogenase (LDH) at admission; U/L (upper limit 250) – Median [IQR] | 381·00 | [229·25] | 342·00 | [180·00] | 566·00 | [308·00] | <0·001 |
| d-dimer at admission; μg/mL | |||||||
| (upper limit 0·25) -Median [IQR] | 0·79 | [3·02] | 0·65 | [1·88] | 2·61 | [5·59] | <0·001 |
| d-dimer at admission | |||||||
| ≤ 2·5 μg/mL | 374 | 70·04% | 312 | 76·28% | 62 | 49·60% | <0·001 |
| > 2·5 μg/mL | 160 | 29·96% | 97 | 23·72% | 63 | 50·40% | |
| d-dimer at outcome; μg/mL (upper limit 0·25) -Median [IQR] | 0.51 | [0·71] | 0·39 | [0·51] | 1·19 | [4·37] | <0·001 |
| Creatinine at admission; μmol/liter | |||||||
| (upper limit 83·88) – Median [IQR] | 79·56 | [26·52] | 79·56 | [35·36] | 83·88 | [38·13] | <0·001 |
| Creatinine at outcome; μmol/liter (upper limit 83·88)- Median [IQR] | 79·56 | [35·36] | 68·63 | [26·52] | 91·5 | [82·35] | <0·001 |
| Creatinine; peak during admission, μmol/liter (upper limit 83·88) – Median [IQR] | 76·25 | [38·13] | 76·25 | [35·36] | 102·94 | [91·5] | <0·001 |
| Arterial hypertension (Yes; n,%) | 276 | 46·94% | 198 | 43·81% | 78 | 57·35% | 0·006 |
| Diabetes mellitus (Yes; n,%) | 95 | 16·16% | 58 | 12·83% | 37 | 27·21% | <0·001 |
| Chronic respiratory disease (asthma, COPD) | |||||||
| (Yes; n·%) | 114 | 19·39% | 84 | 18·58% | 30 | 22·06% | 0·369 |
| Previous rheumatic disease (Yes; n,%) | 28 | 4·76% | 20 | 4·42% | 8 | 5·88% | 0·484 |
| Cancer (Yes; n,%) | 77 | 13·10% | 53 | 11·73% | 24 | 17·65% | 0·073 |
| Previous cerebral ischemic disease (Yes; n,%) | 21 | 3·57% | 12 | 2·65% | 9 | 6·62% | 0·037 |
| Chronic liver disease (Yes; n,%) | 24 | 4·08% | 18 | 3·98% | 6 | 4·41% | 0·824 |
| Chronic kidney disease (Yes; n,%) | 22 | 3·74% | 12 | 2·65% | 10 | 7·35% | 0·011 |
| Chronic cardiac disease, including heart failure (Yes; n,%) | 133 | 22·62% | 78 | 17·26% | 55 | 40·44% | <0·001 |
| Smoker (n,%) | |||||||
| Never smoked | 508 | 86·39% | 387 | 85·62% | 121 | 88·97% | 0·330 |
| Active smoker | 68 | 11·56% | 54 | 12·00% | 14 | 10·29% | |
| Former smoker | 12 | 2·04% | 11 | 2·43% | 1 | 0·74% | |
| PaO2/FiO2 (PAFI), at admission, mmHg Median [IQR] | 313·00 | [98·00] | 319·00 | [71·00] | 223·00 | [147.00] | <0·001 |
⁎
P-value· χ2 test (qualitative variables) or Mann-Whitney U test (quantitative variables) comparing patients· death or alive. Abbreviations: years, yrs; days, d.; interquartile range, IQR.
We used the next CsA oral formulations: Sandimmun Neoral (Novartis) and Ciqorin EFG (Teva), 50 mg, or 100 mg modified capsules taking with food. The intravenous formulations were 50 mg/ml or 250 mg/5 ml, Sandimmun (Novartis). Patients avoid high fatty meals. We designed a CsA low-dose schema, adjusted by patients’ weight (< 5 mg/kg/day) because acute renal failure is related to higher doses of CsA.
We started CsA either as a salvage therapy between the first 72 h after admission in non-responder patients to other drugs or as soon as possible, according to the attending physician. We set the CsA therapy duration in 7-10 days or up to 21 days in the most severe cases.
We took into account some relevant points in the CsA use. We selected a target plasma CsA concentration (ng/ml) levels between 83·2 – 374·4 nmol/liter – upper allowed limit up to 600 – 1050 nmol/liter [26]. CsA steady-state tissue concentration takes place after a minimum accumulated dose of 300 mg (300 mg m.c.d.), approximately. If the patient took CsA beyond one week, we assessed plasma levels systematically.
We recorded the next adverse side effects of CsA: new-onset arterial hypertension or worsening of previous controlled measures, acute renal injury defined as an increase in serum creatinine above 0·5 mg/dl, or more, within the first 48 h of its use, and above previous serum creatinine level; hypokalemia; and an increase in transaminases more than 2·5 times the upper limit of the normal range.
We designed a withdrawal of CsA in those patients admitted to the ICU. Then, intravenous dexamethasone was prescribed according to formerly published data in acute respiratory distress syndrome.
The use of azithromycin, or other concomitant antibiotics, was not recorded. The impact of these drugs on the evolution of severe COVID-19 might be marginal.
For the present study, we compared patients who received a total cumulative dose of 300 mg 300 mg (m.c.d.) (300 mg m.c.d.), or more, of CsA during their in-hospital admission with those who did not receive CsA or received a total cumulative dose of less than 300 mg. Some drugs (hydroxychloroquine, CsA, glucocorticosteroids) might complete at home after hospital discharge, according to the physician’s criteria. All patients who were discharged, and able to complete the dose of CsA by mouth, were also included in the cohort of CsA 300 mg (m.c.d.).
2.5. Statistical analysis
Continuous variables were presented as median [interquartile range, IQR] or mean, ± standard deviation, SD – according to the Kolmogorov-Smirnov test- and absolute (n) or relative (%) frequencies in categorical variables. We applied the χ2 test and Student’s t-test (or Mann-Whitney test if variables have non-normal distribution) to assess the differences in the clinical outcome, radiologic scores, biochemical values, and treatments. The missing values on the database (missing completely at random) were excluded from the analysis – although not the whole case/patient. Thus, no additional technique was used to fill these gaps in current clinical research.
A binary logistic regression model appraised the risk factor for in-hospital mortality. The factors included in the univariate model were those with any variable with a p-value < 0·1. Then, to estimate the odds ratios and 95% CI for each factor – applying the Wilson method for calculating CI [27] – a multivariate model was run.
We then aimed to assess the association between different drugs and in-hospital mortality in patients admitted with COVID-19 using a Kaplan-Meier method and log-rank test. While multiple combinations might be possible and considering a retrospective analysis, we appraised the effect of receiving, or not, each of the available drugs included in the protocol (combined or alone): hydroxychloroquine, lopinavir/ritonavir, CsA, glucocorticoids, and tocilizumab.
All statistical analyses were conducted using SPSS software, version 23·0 (IBM Corp; USA.) and considering a significance p-value <0·05.
3. Results
We collected data on a total of 607 patients (Fig. 1S). The median age in the cohort was 69 years [22]; 34·98% were female (table 1). At the end of the study period, 194 (31·92%) remained in the hospital and were followed until 12th May 2020. During the in-hospital follow-up, 466 patients survived (76·08%) and 141 died (23·2%) – with a strong weight on the older ones (Fig. 1). Table 2 shows the in-hospital mortality relative to the given therapy. The median in-hospital overall length of stay was 8·0 [9·0] days.
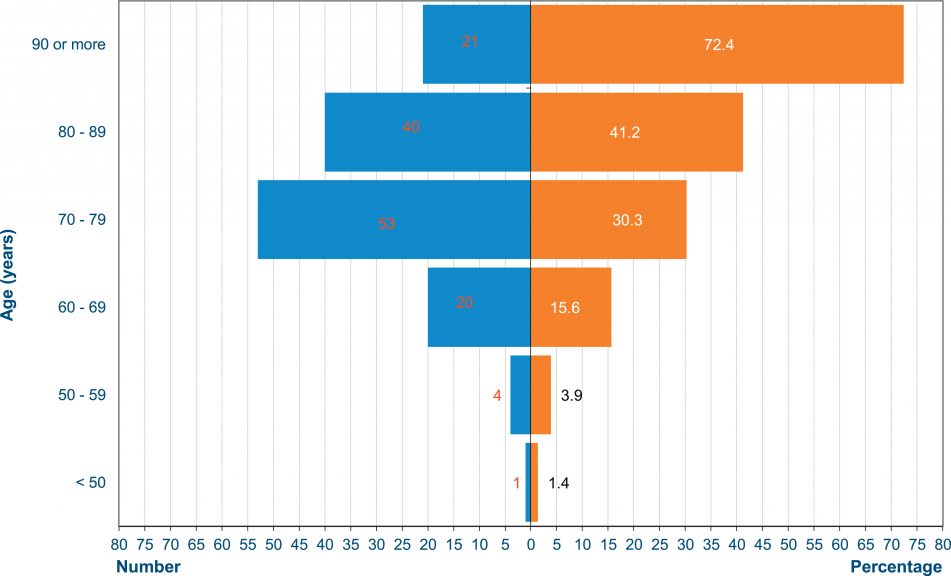
Fig. 1. Crude mortality rate (percentage, orange boxes, absolute numbers, blue boxes) according to age of the patients included in the study.
Table 2. In-hospital mortality according to prescribed therapy.
| Treatment | All patients (n,% all) | Mortality (n,% treated) | IC 95% | P value* | |||
|---|---|---|---|---|---|---|---|
| Hydroxychloroquine – before admission | |||||||
| Yes | 65 | 10·71% | 2 | 3·08% | 0·85% | 10·54% | <0·001 |
| No | 542 | 89·29% | 139 | 25·65% | 22·15% | 29·48% | |
| Hydroxychloroquine | |||||||
| Yes | 558 | 91·93% | 127 | 22·76% | 19·47% | 26·42% | 0·356 |
| No | 49 | 8·07% | 14 | 28·57% | 17·85% | 42·41% | |
| Tocilizumab | |||||||
| Yes | 132 | 21·75% | 44 | 33·33% | 25·86% | 41·75% | 0·002 |
| No | 475 | 78·25% | 97 | 20·42% | 17·04% | 24·28% | |
| Lopinavir/ritonavir | |||||||
| Yes | 487 | 80·23% | 111 | 22·79% | 19·29% | 26·72% | 0·608 |
| No | 120 | 19·77% | 30 | 25·00% | 18·11% | 33·44% | |
| Cyclosporine A | |||||||
| Yes | 253 | 41·68% | 36 | 14·23% | 10·46% | 19·07% | <0·001 |
| No | 354 | 58·32% | 105 | 29·66% | 25·14% | 34·62% | |
| Glucocorticoids | |||||||
| Yes | 159 | 26·19% | 46 | 28·93% | 22·45% | 36·41% | 0·109 |
| No | 448 | 73·81% | 95 | 21·21% | 17·67% | 25·23% |
⁎
P-value· χ2 test comparing the mortality between treated patients, or not. ¶ stable plasma dose >300 mg.
The number of patients admitted to the ICU was 49 (8·07%) (table 2S). Of them, 45 (7·41%) required invasive mechanical ventilation, 6 need continuous renal replacement therapy, and 3 had extracorporeal membrane oxygenation (ECMO) therapy. The ICU mortality rate was 17·02% (24 patients).
The median PAFI at admission was 313·0 [98·0] mmHg, with a statistically significant difference between survivors and non-survivors (319·0 [71·0] mmHg vs 223·0 [147·0] mmHg, respectively).
Table 1 shows comorbidities, clinical outcomes, and laboratory parameters for the survivors and non-survivors datasets.
The most common comorbidities were: hypertension (276 [46·94%]), mellitus (95 [16·16%]), chronic cardiac (133 [22·62%]) and respiratory (114 [19·39%]) diseases.
Hydroxychloroquine – prescribed as an intention to treat a mild stage of COVID-19 and in those without any known autoimmune disease – was given before hospital admission in 65 (10·71%) patients. During hospitalization, 558 (91·93%) patients received hydroxychloroquine, 487 (80·23%) antivirals (lopinavir/ritonavir), 132 (21·75%) tocilizumab, 159 (26·19%) glucocorticoids, and 253 (41·68%) CsA 300 mg m.c.d. mg m.c.d.”?> – alone, or in different combinations.
We did not find any differences PG (in days) from the initial symptoms of the SARS-CoV-2 infection to the start of the anti-inflammatory therapies (glucocorticoids, tocilizumab, or CsA 300 mg m.c.d.) (Table 3S).
In the univariate logistic regression model, factors associated with in-hospital death were: age, arterial hypertension, diabetes mellitus, cancer, previous cerebral ischemic disease, chronic cardiac disease (including heart failure), higher radiological score at admission, PAFI at admission, receiving invasive mechanical ventilation, previous therapy with hydroxychloroquine, treatment with tocilizumab, glucocorticoids or CsA 300 mg m.c.d.; lactate dehydrogenase (LDH), and C-reactive protein (CRP), creatinine at admission, levels of ferritin above 1000 μg/liter, and d-dimer > 2·5 μg/mL.
The risk of death in the multivariate model revealed increasing odds of death with older age (for every year of age, the odds ratio was 1·15, [95% CI 1·11 – 1·2]); CRP at admission (for every increase of 10 mg/L, the observed risk of death was 7% higher, 1·07, [1·04 – 1·10]); d-dimer > 2·5 μg/mL (1·99, [1·03 – 3·86]); and diabetes mellitus (2·61, [1·19 – 5·73]). The PaO2/FiO2 at admission also showed a statistical significance (per every 1 mmHg, 0·99, [0·98 – 0·99]) – for every extra unit of PAFI in any given patient, compared to another with lower values, the risk of death decreased by 1% (Fig. 2).

Fig. 2. Univariate and multivariate logistic regression model of the risk factors for in-hospital death, including baseline comorbidities, laboratories parameters and available therapies.
Among the prescribed therapies, two of them kept the statistical significance, confirming the observation of the crude mortality rate (Table 4S). On the one hand, tocilizumab therapy showed an increased odd of death (2·4, [1·13 – 5·11], p = 0·023). On the other hand, CsA 300 mg m.c.d. was associated with a significant decrease in the observed mortality (0·24, [0·12 – 0·46], p<0·001) (Fig. 2). In other words, the odds of death were 0.24 times [one-fourth] in the CsA 300 mg m.c.d. group comparing to those cases who took any other therapy, including CsA < 300 mg m.c.d., after adjusting for age, tocilizumab therapy, CRP at admission, d-dimer > 2·5 μg/mL, mellitus, and PaO2/FiO2 at admission. The side effects attributed to CsA 300 mg m.c.d. were: arterial hypertension, acute renal failure, acute gouty arthritis (Table 5S); in any case, no permanent organ dysfunction arose. The median total given doses of CsA was higher among survivors than in non-survivors (750 [650] mg vs 500 [375] mg, p<0·001).
Fig. 3 (A-D) shows the impact on mortality of hydroxychloroquine, tocilizumab, lopinavir/ritonavir, and glucocorticoids. The observed median time of survival in the Kaplan-Meier curve was different (p<0·001) in patients treated with CsA 300 mg m.c.d., comparing to those cases with any other therapy, including CsA < 300 mg m.c.d. (Fig. 4, Table 6S).
Fig. 3. Observed cumulative in-hospital death, or alive, according to each given drug available in the protocol. Shading represents 95% confidence intervals. Panel A, Hydroxychloroquine. Panel B, Tocilizumab. Panel C, Lopinavir/ritonavir. Panel D Glucocorticoids.
Fig. 4. Observed cumulative in-hospital death, or alive, according to steady-stable dose of Cyclosporine A. Shading represents 95% confidence intervals.
4. Discussion
The present retrospective cohort study found well-known risk factors associated with in-hospital mortality in COVID-19 pneumonia, analogous to previous studies of similar scope [28], [29]. In this setting, we observed an important finding: decreased odds of in-hospital death in patients treated with CsA 300 mg c.d. Namely, the odds of death in those cases not reaching minimum CsA 300 mg m.c.d. were 4·2 times higher compared to those patients who achieved this minimum doses or higher than in the CsA 300 mg m.c.d. group [30]. mg m.c.d. were 42 times higher compared to those patients who achieved this minimum doses or higher.”?> This finding might suit other populations with severe COVID-19, either in Spain or abroad. No data suggest any differences in NK-κB activity related to race or gender.
To our best knowledge, this is one of the first studies to describe the clinical use of CsA and its impact on mortality in severe COVID-19. We informed the National Health Authorities of the use of CsA in the current protocol, and a prospective study is in development. The design of the study does not allow head-to-head comparison among treatments used in COVID-19.
Few indirect data published recently might support the potential therapeutic effect of CsA in SARS-CoV-2 infection. Some researches reported a low incidence of COVID-19 among those affected by rheumatic diseases [31] or might have a better prognosis in kidney transplant recipients [32]. Other authors even proposed CsA itself as a potential therapeutic drug in COVID-19 [33,34]. CsA is a unique immune inhibitory drug as it blocks NF-κB through inhibition of calcineurin. This noticeable mechanism of CsA might interfere with the initial step of the cytokine storm release in severe COVID-19 [19].
As mentioned above, CsA activity against CoVs grounds on pre-clinical data [35,36] – some were recently replicated in a SARS-CoV-2 infection model [37]. In this sense, the non-structural protein type 1 (nsp1) of CoVs interacts with its counterpart immunophilin molecules. This immune pathway plays a central role in the activation of immune cells. Overexpression of nsp1 in CoV infection steadily increases the signaling of this pathway [18]. CsA is a potent blocker of the growth of CoVs of all genera, including SARS-CoV, human CoV-NL63 and CoV-229E in cell culture. This inhibitory effect occurs at low, non-cytotoxic concentrations of the drug [38] – FK-506 (tacrolimus) shows similar findings, although perhaps not with such broad a spectrum as CsA [39].
The CsA-CypA complex can sequester and inhibit calcineurin (a calcium-calmodulin-activated serine/threonine-specific phosphatase), which would prevent the nuclear translocation of NFAT, and finally, the expression of genes implicated in the immune response to the infection, such as IL-2, IL-12, or TNF-α [40,41]. Accordingly, CsA might convey an anti-inflammatory cytokine profile by inhibiting NFAT (thus, increasing IL-10 secretion, and reducing IL-12 and TNFα release). Otherwise, CypA regulates the activation and signaling of NF-κB too. The actions and role of NF-κB go beyond T cell regulation. CsA also impacts on the function and maturation of innate immune cells, including dendritic cells (DC), macrophages, and neutrophils. This drug inhibits DC expression of IL-2 and maturation markers, CD80, CD86, CD40, which in turn reduces T cell proliferation. Furthermore, another property of CsA is the ability to inhibit the mitochondria permeability transition (MPT) pore and prevent the release of danger-associated molecular patterns (DAMPs) – downregulating the secretion of IL1β and type I interferons [41].
Some differences in the activity of NF-κB among individuals could help to explain the impact of CsA on mortality in the current study. It is noteworthy to underscore the previous description of an age-dependent NF-κB activation connected with systemic inflammation and impaired endothelial-dependent dilatation. On the one hand, NF-κB plays a pivotal role in mediating vascular endothelial dysfunction in overweight and obese middle-aged and older humans (pro-inflammatory phenotype) [42]. On the other hand, an inflammatory activation of NF-κB, and oxidative stress, cause vascular insulin resistance and may contribute to endothelial dysfunction in diabetes mellitus [43].
An over activation of NF-κB related to age (inflammaging) might explain the severity of COVID-19 in the elderly – in opposite to young adults without any comorbidity, including obesity. It might also explain why most hospitalized patients are older [44].
To minimize expected adverse side effects of CsA, we used it with the following precautions: short time of treatment -maximum 3-weeks-, low-dose, weight-adjusted, and compatible with other available drugs.
Considering the time required for CsA to reach a biological therapeutic effect, we examined at least an accumulated dose of 300 mg of CsA to make clinical endpoint comparisons among patients. In fact, in a recent study on the use of an inhibitor of Bruton tyrosine kinase in COVID-19 pneumonia, a 3-day therapeutic effect was also reported [45].
During our experience in the treatment of COVID-19, CsA use moved swift from salvage therapy in refractory cases to initial therapy at triage. Nevertheless, some other relevant aspects might have influenced our in-hospital mortality results. Since the beginning of the SARS-CoV-2 epidemic, our protocol recommended the use of subcutaneous prophylactic low-molecular-weight heparin (bemiparin 3·500 UI q.d.). Full anticoagulation started if we diagnosed a venous thromboembolic disease. Some selected cases might change to the anticoagulation schema if their respiratory situation did not improve, d-dimer levels reached extreme values, or imaging techniques were negative to detect pulmonary embolism or deep venous thrombosis.
Some authors have prior reported an increase in plasma levels of IL-6 in COVID-19 patients with acute pulmonary damage [46]. Thereupon, blocking the action of this cytokine with tocilizumab, or other similar agents, was proposed as a theoretical therapeutic approach for COVID-19 pneumonia [11,17]. But IL-6 is not the only marker of inflammation in COVID-19. Other inflammatory parameters have a robust association with mortality, such as d-dimer > 2·5 μg/mL or levels of CPR above 200 mg/L47. We did not measure IL-6 plasma levels in our patients, including those receiving tocilizumab. Our hospital does not currently have access to rapid-turnaround cytokine measurements. However, different studies found that IL-6 does not appear to be a determinant prognostic factor in COVID-19 [29]. A common clinical problem exists with the cytokine release syndrome and the CAR T-cells therapy: the optimal time to administration of tocilizumab is unclear if only guided by IL-6 plasma levels. A clinical grading scale, together with other widely available inflammatory markers, might be more flexible and accurate [48]. Moreover, after tocilizumab scheduled, the plasma levels of IL-6 do not help patient follow-up: after blocking the IL-6 receptor, the levels of IL-6 become even higher or do not drop immediately [11].
Tocilizumab was not associated with a benefit in mortality rates in our patients, even adjusting for dose and the severity of hypoxemia [49]. Our observations underscore the need of releasing the results of ongoing clinical trials to clarify these findings. Noteworthy, in our patients, the time from the beginning of symptoms to the initiation of tocilizumab or CsA was similar (11 days).
The finding of no benefit in glucocorticoids in a retrospective study was pointed out previously. On the contrary, recently some research groups reported a positive effect of glucocorticoids on COVID-19 mortality [50]. Although drawing a categorical conclusion about the systemic benefit of glucocorticoids in severe COVID-19 might be not exactly accurate [51].
In general, we used glucocorticoids in some cases and dexamethasone in all ICU admissions. We also treated with this glucocorticoid some selected patients who were admitted to general wards. The doses of glucocorticoids varied but preventing the higher ones [47].
Our study has some limitations. The research was carried out in a single academic center and had an observational and retrospective design. Thus, unmeasured confounding factors might influence our findings – including a time-varying effect (if any) of previous treatment or other covariables. What’s more, even the natural evolution of the disease itself, as well as the immortal time bias, might have an impact on our results. A few aspects of the use of CsA on COVID-19 pneumonia should assess in future research, such as the drop in inflammatory parameters, rise in the PAFI, or the incidence of thromboembolic disease. We did not record some variables systematically as obesity, race, and ethnicity in our clinical records. For this reason, we decided to exclude them for statistical analysis purposes. For this reason, we decided to exclude them for statistical analysis purposes.
In conclusion, the NF-κB and NFAT appear to be pivotal mediators of pro-inflammatory gene induction after infection of SARS-CoV-2. Both might play a central role in the hyperinflammation state observed in severe COVID-19 patients. Our findings suggest a possible benefit of CsA on in-hospital mortality among patients with severe COVID-19. These findings might support the hypothesis to include CsA in future therapeutic protocols if prospective, well-designed clinical trials confirm the current results.
Related: