
Source:Rounding The Earth Author: Mathew Crawford
Part 1 of the interview:

A few days ago on their DarkHorse Podcast, Bret Weinstein and Heather Heying discussed the suppression of the use of ivermectin as treatment for COVID-19, concluding that this is the “crime of the century”. Shortly thereafter, Bret invited Dr. Pierre Kory on for an in depth discussion.
Let’s break down everything they covered including what I think they get right and exactly what I think they get wrong.
Dr. Kory discusses how the Front Line COVID-19 Critical Care Alliance (FLCCC) formed as an organization for motivated doctors to go after what might be called “empiric medical treatments” of COVID-19. If I understand correctly, this effort began when highly successful and well published Dr. Paul Marik began examining protocols for patients experiencing sepsis. Dr. Kory started working with Dr. Marik soon after, and the circle expanded to doctors who found good use for corticosteroids and blood thinners in treatment of some COVID-19 patients.
Dr. Kory spoke in front of the senate in May, 2020 and received pushback for his witnessing of these therapies that are now in fact standard of care (SOC) for COVID-19 patients.
So far, so good. The FLCCC held firm on these views, was vindicated by the evidence, and likely saved many lives due to these revelations.
Dr. Kory then discusses the progression of COVID-19 including the way that around days 5-8, a proportion of patients begin to have low oxygen when a macrophage (scavenger cell) begins to attack the lungs in an autoimmune reaction, causing substantial inflammation and injuring the lung. During the early months of the pandemic, many of these patients were being marched quickly to ventilators without ever being treated in any way.
As an aside, Dr. Marik warned early in the pandemic that the ventilators made the inflammation worse.
At some point Bret engages Dr. Kory in a good discussion of the history of medicine and the value of pattern recognition [that seems to be lost in the jungle of today’s medical science regime]. Bret laments a similar loss of intuition and art in his own field. The two seem to agree that we’re living in an era of intellectual authoritarianism, which is a term I’ve also used. This leads into a discussion of the dangers of censorship and how shutting down discussion of the views of actual clinical doctors is antithetical to science. So, up to this point, I’ve got no problem at all with this interview. In fact, I endorse these messages. Moving on…
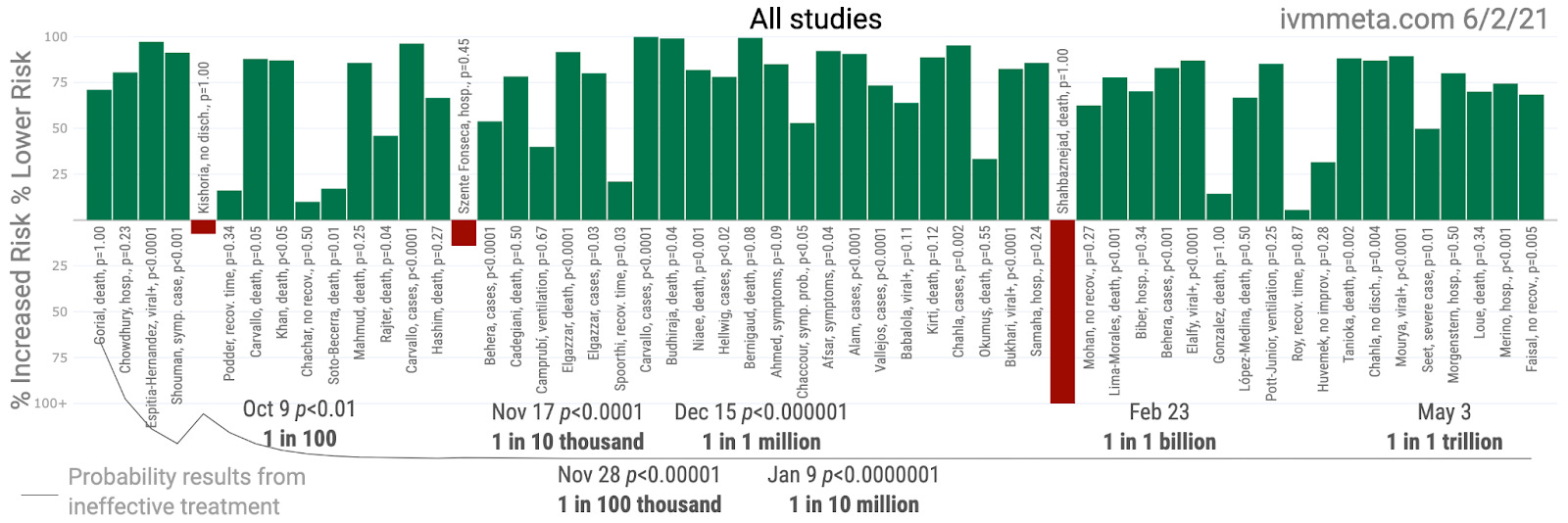
At around 31:45, Dr. Kory gets into ivermectin (IVM) and points out that there is nothing but positive evidence suggesting IVM’s efficacy in treating COVID-19.
Ah, but this simply isn’t true! While most of the 56 studies on IVM demonstrate highly positive results (that are remarkably similar), not every study showed positive benefit. See for yourself!
The discussion then covers IVM’s excellent historical safety record and the rationale for the experiments in usage of IVM in Peru where SARS-CoV-2 infection rates plummeted where IVM was used. The FLCCC carefully studied these results, including this paper published in May, 2020, the FLCCC moved closer to including IVM in its top priority recommendation list.
During this discussion, Bret says that in a perfect world, we would have “gold standard RCT” evidence to move forward with. While I’m not going to dwell on it, I will point to my articles here and here as to why I think we should abandon that perspective. But that is aside from my critique of “the crime of the century” and there is no doubt at all that RCTs help an evidence pool prior to the accumulation of a solid few-thousand clinical data points.
Around 49:00, Dr. Kory sort of slides in a suggestion that the reason the IVM evidence is not accepted as demonstrative is that none of the numerous RCTs among the studies above are “a big pharma-conducted…or North American-Western conducted trial”. Bret refers to this perspective by authorities as “obstructionist”, which is something I’ve believed about the “official” responses to IVM for the better part of a year now. But I believe we are now publicly into an argument not simply for malfeasance, but also for ethnocentric gerrymandering of standards. Perhaps the pharma-government-NGO complex is truly where real white supremacy lives? I might reframe that as an argument of the cancer of corporatism.
Bret and Dr. Kory then dance around conspiracy theory while pointing out that some IVM detractors are honest brokers with poor perspectives. Entirely fair. This leads into a moment when Dr. Kory points out that the RCTs of IVM often show greater effect sizes than the observational studies. Since so many of the IVM RCTs are early treatment studies, this matches my observation that early treatment effects are being under-reported due to poor statistical modeling.
Part 2 of the interview:

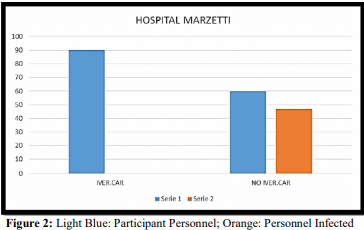
The conversation veers into the fact that both Bret and Dr. Kory sourced IVM the moments they understood the implications and that IVM alone would end the pandemic. Dr. Kory points out the hefty differential (0% to 58%) in infection rates in an IVM prophylaxis study, and the natural experiments in India where states using IVM are dramatically lower than those that are not, including one state that banned it. We do not disagree, and I called that one the moment I heard about the spike in India.
I know you must be wondering where I disagree with this crew. Here I urge patience because this topic is of such critical importance…
At around 1:16:00 the conversation veers into a discussion of corruption. There is discussion of the level of sinister actors, including sociopaths, and the possibility of benign neglect, blinded by good intentions. This conversation should be taking place in more quarters than it has been to date. The conversation covers varying levels of illogic in the way the vaccines are being favored as the entire solution when IVM could substantially contribute to herd immunity. Bret then points out that delaying treatment is malpractice (which it is).
Bret and Dr. Kory also discuss the strangeness of the fact that the vaccines focus exclusively on the spike protein, which risks variant escape, whereas IVM seems to work universally on all the SARS-CoV-2 strains.
Additional and repeated points over the middle of the interview:
IVM seems to be extremely safe and effective by essentially all accounts.
Fluvoxamine and some other drugs may work for some patients, but have side effects.
The COVID-19 vaccines have a variety of real risks, and it’s not “anti-vaxx” to take those into account in a cost-benefit/risk-benefit analysis.
Natural experiments in Africa showed that nations with anti-parasitic public health programs had much lower rates of COVID-19 than those that did not, which is suggestive of IVM efficacy since it is a centerpiece of such programs.
IVM acts as both an antiviral and anti-inflammatory agent.
Adverse events for IVM are “exceedingly rare”.
The “Army of Public Health” has not been doing the work to figure all this out, which looks on face like a runaway conflict of interest, with profits as the primary goal.
The recommendations for the use of corticosteroids advise too low of a dose, which may be resulting in unnecessary deaths.
I’ve got no beef with any of these observations and I’m going to dodge summarizing the last 35 minutes of the conversation so that I can make the necessary point, then go to bed. It’s past 3 AM in Texas, and sleep is health, so here goes…
Bret, Pierre, Heather, and a large number of internet pundits make a great case that suppression of ivermectin is a large, gross, and inhumane crime. However, this is not the “crime of the century”. The crime of the century is far larger, or rather more systemic. It includes the following and much more:
- The suppression of all early treatment for COVID-19, including ivermectin, hydroxychloroquine, simple vitamin packs, companion medications, and others.
- The mortgage bond crisis which destroyed so much wealth worldwide that it was probably responsible for many millions of deaths, and led to increased centralization of wealth and power may precede the aforementioned crimes.
- The threats toward and corruption of the free media, not that it was ever fully free of corruption, of course, through the torture and exile of major whistleblowers, sets the stage for so many crimes of the century that we should view it, too, as a mass crime on that level.
- I could go on and plan to in future articles, and some of the topics will shock many and be difficult to absorb, but we have moved into a world state of endemic corruption in which the kunlangeta have organized their control on a level that has trained into a significant portion of humanity a dehumanized view of “others” that will continue to manifest as crime of the century after crime of the century until we figure out how to push the kunlangeta off the ice.
Finally, I would be remiss if I did not point out the numerous ways that IVM can be obtained.
Some of these sources do provide IVM as prophylaxis so that you don’t have to depend on horse paste, which just sort of feels weird, even if it might work just as well. You are welcome.
The Chloroquine Wars Part VIII – Hydroxychloroquine’s Safety Profile and a Cost-Benefit Analysis
The Chloroquine Wars Part X – A Discussion of the Insanity of the Chloroquine Wars
The Chloroquine Wars Part XI – See No Good, Hear No Good, Speak No Good
The Chloroquine Wars Part XII – Manufactured Fear During Hydroxychloroquine’s Trump Moment
The Chloroquine Wars Part XIII -A Clockwork Orange Man
The Chloroquine Wars Part XIV – How to Rig Research: Surgisphere Part I
The Chloroquine Wars Part XVII – Why the Story About India’s April COVID-19 Spike is All Wrong
The Chloroquine Wars Part XV – How to Rig Research: Surgisphere Part II
The Chloroquine Wars Part XIX – Historical Failures of Public Health Authorities
The Chloroquine Wars Part XX – Why The Early Treatment Data is Better Than Anyone Imagines
Doctor Didier Raoult Part I: Where We Are Now -The Chloroquine Wars Part XXV