
Source: Medicine Uncensored
by James M Todaro, MD (Columbia MD, @JamesTodaroMD)
August 6, 2020
MEMORANDUM
TO: Jenny Beth Martin, Founder, Second Opinion Project
TO: Interested Parties
FROM: James Todaro, MD, Founder Medicine Uncensored
DATE: August 6, 2020
RE: Risk analysis of heart rhythm problems in early, short-term treatment of COVID-19 with Hydroxychloroquine
Summary
This memo is a response to the FDA’s July 1, 2020 update on the use of hydroxychloroquine for COVID-19, “FDA cautions against use of hydroxychloroquine or chloroquine for COVID-19 outside of the hospital setting or a clinical trial due to risk of heart rhythm problems”. [1]
Hydroxychloroquine has been safely used in millions of patients with approximately 20 reported deaths worldwide attributed to its use over the past 50+ years. In the setting of a short course of treatment with hydroxychloroquine for COVID-19, it is highly unlikely that fatal cardiac cases are from hydroxychloroquine use, especially during the early stage of COVID-19. It is far more likely that the disease itself is the cause of arrhythmias and cardiac injury during the hyperinflammation phase of COVID-19.
Detailed Analysis
The July 1 update directs to a “Pharmacovigilance Memorandum” dated May 19, 2020, by the Department of Health and Human Services, Public Health Service, Food and Drug Administration, Center for Drug Evaluation and Research, and Office of Surveillance and Epidemiology. [2]
In Table 4 of this pharmacovigilance memorandum, the above agencies report 347 cases of adverse events and 77 deaths in patients receiving hydroxychloroquine in the setting of COVID-19. In Table 5, it shows that 17 of the fatal cardiac cases were “possibly/probably associated” with hydroxychloroquine.
It is likely that the majority (or perhaps all) of these 17 cardiac deaths are actually a result of the disease course of COVID-19 and not from hydroxychloroquine usage.
In the last 50+ years of use, hydroxychloroquine has been attributed to an infinitesimal number of deaths, including those of cardiovascular nature. From the years 1963 to 2017, there are only 50 reported adverse events and 12 reported deaths attributed to cardiac toxicity from routine dosing of hydroxychloroquine (not including intentional overdosing which I will address later). [3] Furthermore, the median daily dose and duration of treatment among those 50 adverse events are 400mg of hydroxychloroquine taken daily for 8 years. Millions of patients have taken hydroxychloroquine for malaria treatment and prophylaxis as well as autoimmune disorders including rheumatoid arthritis and systemic lupus erythematosus over the past half a century.
Hydroxychloroquine is routinely used by rheumatologists in patients with many comorbidities (including cardiovascular), and hydroxychloroquine treatment is not typically discontinued in patients during acute infections with influenza virus and the various viruses that make up the “common cold.” Moreover, there is not a single infection that is documented to be an “absolute” or “relative” contraindication to taking hydroxychloroquine. [4] It would be highly unusual for the SARS-CoV-2 infection to be the first infection on this list. It is even less likely considering the short duration of treatment and extremely low cumulative dose when used for COVID-19.
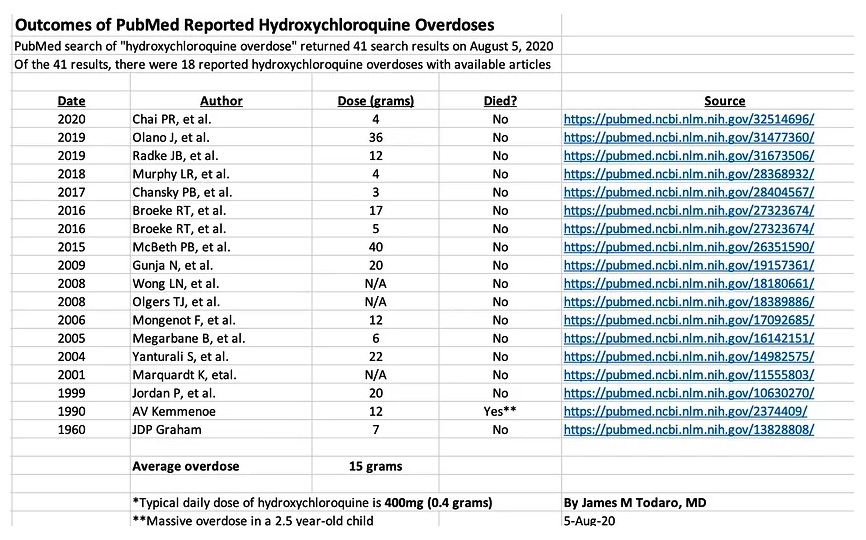
As a testament to hydroxychloroquine’s safety profile, even in situations of intentional overdosing, hydroxychloroquine is usually not lethal with urgent medical intervention. In the 18 reported cases of hydroxychloroquine overdosing in a PubMed literature search (n=41 results for “hydroxychloroquine overdose” with n=18 described cases of overdoses with available articles), most patients survive even after consuming 50-100x the standard dosing. The overdoses among these 18 patients ranged from 3g to 40g with a mean dose of 15g. For reference, 15g is the consumption of seventy-five 200mg tablets. The only reported death in this PubMed literature search was in a 2 ½-year-old boy who consumed 60 tablets of 200mg hydroxychloroquine. (See table below)
It could be argued that hydroxychloroquine is even safer than Tylenol, both in routine dosing and cases of intentional overdosing. Analysis of national databases estimates there to be 26,000 hospitalizations and 458 deaths annually from acetaminophen (e.g. Tylenol) in the USA alone. [5] On the other hand, including both deaths from routine dosing as well as intentional overdosing, there are approximately only 20 reported deaths attributed to hydroxychloroquine as of the year 2017. While it can be argued that acetaminophen is more commonly taken than hydroxychloroquine, it is important to realize that there are over 5 million hydroxychloroquine prescriptions annually in the USA alone. [6] Yet, the cumulative reported 20 deaths from hydroxychloroquine are from use worldwide over the past 50+ years.
For the above reasons, it is highly unlikely that the fatal cardiac cases in the FDA’s pharmacovigilance memorandum are a result of hydroxychloroquine use. It is far more likely that the natural disease course of COVID-19 is the cause of the arrhythmias and cardiac injury. Multiple studies show that between 7.2% and 19.7% of hospitalized COVID-19 patients experience cardiac injury from this disease regardless of hydroxychloroquine use. Of those with cardiac injury, arrhythmias are common, occurring in about 25% of patients with cardiac injury. [7,8,9,10] Furthermore, serious and lethal arrhythmias were not determined to be associated with hydroxychloroquine use in a prospective study of COVID-19 patients published in a journal by the American Heart Association. [11]
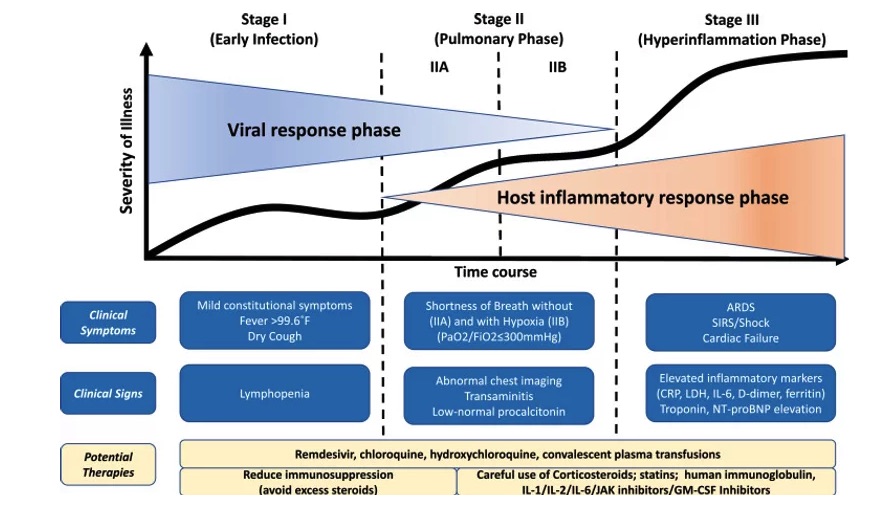
Lastly, since March of this year, physicians treating COVID-19 patients have continually advocated use of hydroxychloroquine in early treatment of COVID-19 (within 4 days of symptom onset). During this early infection stage (Stage I), symptoms are present in the absence of any cardiac injury, which does not typically occur until Stage III of the disease. As shown in the diagram below, elevated troponin—a marker for cardiac injury—does not appear until the hyperinflammation phase in Stage III. [12] Thus, it is even less likely for hydroxychloroquine to cause adverse cardiac events when used in early treatment of COVID-19.

In conclusion, hydroxychloroquine has been safely used in millions of patients with approximately 20 reported deaths worldwide attributed to its use over the past 50+ years. In the setting of a short course of treatment with hydroxychloroquine for COVID-19, it is highly unlikely that fatal cardiac cases are from hydroxychloroquine use, especially during the early stage of COVID-19. It is far more likely that the disease itself is the cause of arrhythmias and cardiac injury during the hyperinflammation phase of severe cases of COVID-19.
References
[3] https://pubmed.ncbi.nlm.nih.gov/29858838/
[5] https://pubmed.ncbi.nlm.nih.gov/16294364/
[6] https://clincalc.com/DrugStats/Top300Drugs.aspx
[7] https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30183-5/fulltext
[8] https://jamanetwork.com/journals/jama/fullarticle/2761044
[9] https://www.cmaj.ca/content/192/28/E791
[10] https://academic.oup.com/europace/advance-article/doi/10.1093/europace/euaa145/5842075
[11] https://www.ahajournals.org/doi/10.1161/CIRCEP.120.008662
[12] https://www.jhltonline.org/article/S1053-2498(20)31473-X/fulltext
Disclaimer: This memorandum does not constitute medical or professional advice. It is approaching the subject matter from a health policy standpoint. The author shall not be responsible for any errors, omissions, or claims for damages, including exemplary damages, arising out of use, inability to use, or with regard to the accuracy or sufficiency of the information contained in this publication. No responsibility is assumed by MedicineUncensored, authors or editors for any injury and/or damage to persons or property as a matter of product liability, negligence, or otherwise, or from any use or operation of any methods, product, instructions, or ideas contained in the published content. No suggested test, procedure or treatment should be carried out unless under medical supervision.
Related: Dr James Todaro: An Effective Treatment for Coronavirus (COVID-19) – Previously Censored.
Local doctor pushing proven HCQ cocktail treatment for COVID into national debate
Hydroxychloroquine could save up to 100,000 lives if used for COVID-19: Yale epidemiology professor