

Source: Quadrant Author: Emeritus Professor Robert Clancy
Lockdown fever has crept into our lexicon with its destructive effect on the fabric of our lives. We are assured this is but a temporary measure and the only way to keep our community “COVID-free” until vaccine uptake reaches the magical figures of 70 to 80 per cent. Then what? Does it mean the end of COVID-19, or a new way of life? The Doherty Institute has provided “modelling” that informed the government’s decision to plan an end to lockdowns and an opening of our national border. It appears to be basic modelling with limited incorporation of variables. What it does not do is provide a vision of how Australia will “look” once 80 per cent is achieved.
It is not surprising that “modelling” for COVID, indeed modelling for any complex multifactorial event has a poor record. A great imponderable with COVID is the unpredictable appearance and impact of mutant variants that can change the pace of disease by being more aggressive, more transmissible, and/or more resistant to vaccine protection.
The current “third wave” is due to the Delta variant out of India, which delays the host immune response, enabling a higher viral load and greater infectivity. This is similar to the influenza variant which caused the second wave of Spanish flu in 1919 and led to secondary bacterial infection. The Delta variant also stresses waning vaccine immunity but is less lethal than earlier variants. The Lambda variant, identified in Peru in early April, had been isolated in twenty-nine countries by July 2021. It has enhanced viral infectivity and resistance to current vaccines. We await its arrival.
While the pandemic has raged across the northern hemisphere over the last 20 months, Australia has remained relatively free due to its maritime border and efficient public health controls, as it did in 1919 when faced with the Spanish flu. In the US there have been 36 million cases and 630,000 deaths, and in the UK 6 million cases and 130,000 deaths. Over the same period Australia has reported 63,000 cases with just over 1000 deaths (the ongoing tallies can be viewed here). While a cause for concern, this is low compared to most countries. There is now a loss of synchrony with many trading partners, who are hesitantly moving to “business as usual”, while we have created a “bubble” to keep us “COVID-free” with strict border controls, quality “test and isolate” public health measures and “lockdowns”. The success of these methods comes with increasing human and economic cost and distancing from the rest of the world.
This article discusses three difficult but important questions related to our future with COVID-19. First, what does “escape from the bubble” actually mean? Does it mean we return to a pre-COVID world? Second, what is the path to the “escape”? Third, how can we retain this freedom?
MUCH can be learnt from the experiences of countries attempting to move on from Covid restrictions. While none are quite the same as Australia, a review of four countries can contribute general principles that shed light on a future Australian experience. Key characteristics related to COVID exit in the UK, Israel, Sweden and Iceland, are summarised in the table below.
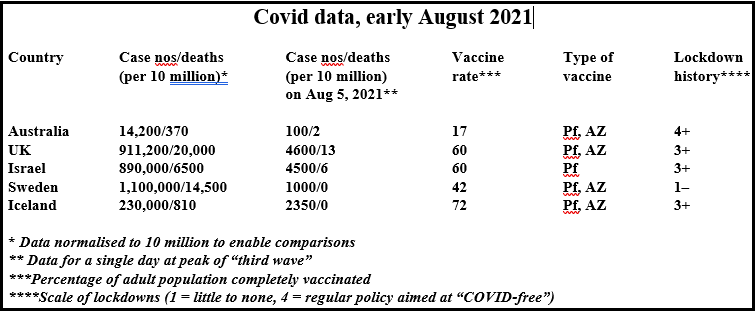
Each of these four countries has experienced three waves of COVID infection, although with different profiles. The shapes of these profiles likely reflect differences in national management strategies. Critical is an understanding that the third or “July-August” wave of infections is due almost entirely to the Delta variant. The following observations can be made:
♦ The UK and Israel had similar levels of infection, although Israel had fewer deaths. Both countries had high vaccination levels (Israel used Pfizer vaccine; the UK used both Pfizer and AstraZeneca). During the third wave both countries experienced similar high infection rates but with few deaths and less hospitalisation. In both countries, those infected irrespective of their vaccination status have been a source of transmission. In Israel, protection waned against mild to moderate disease following vaccination, with little protection at six months, although protection against severe disease remained at 85 to 90 per cent.
♦ Sweden had a more liberal approach to community control, with avoidance of lockdowns. The discrete infection peaks seen in countries using extensive lockdowns were absent. Swedish epidemiologists called this a “front-end loaded” pattern as infections in the “third wave” are lower. This is a level of herd immunity, following both infection and vaccination, and is consistent with emerging evidence that post-infection immunity is broader and more durable than that following vaccination. It is tempting to suggest that natural immunity has an inverse relationship to lockdowns, which are considered by Swedish epidemiologists as “simply buying time”.
♦ The experience in Iceland bears comparison to Australia, as both are islands attempting to be COVID-free. Points of difference are Iceland’s early high-level vaccination rate and a more porous maritime border. Iceland’s tracking data is between that of Australia and Sweden. Iceland’s “third wave” experience is characterised by a high case rate with few deaths.
♦ Normalised to populations of 10 million, the current seven-day averages for Israel and the UK are about 6000 per 10 million population, with about twenty deaths—a six-fold increase over current New South Wales numbers. Both Israel and the UK have vaccination rates of 60 per cent and rising—considerably above Australia. Iceland is overloading its health system with normalised case numbers of 3000 per 10 million, but with no deaths. Sweden is ahead of the game with a flattened “third curve” accredited by their epidemiologists to a high natural immunity attributable to their “front-end loaded” strategy.
The experiences of these four countries recovering their international relationships provide poignant scenarios for Australia. Vaccines will reduce severe disease but with little impact on the number of infections. There will be high rates of mild-to-moderate COVID, with transmission from vaccinated and non-vaccinated subjects causing considerable pressure on our health services. With the chart below reflecting the NSW Health Department’s figures up to September 6 there is no denying that, despite a lockdown in excess of eight weeks, total reported infections continue to rise. The idea of a COVID-free society is over for Australia.

It is likely Australia will continue with significant numbers of COVID cases until the end of the year, when the 80 per cent vaccination rate is expected. Greater movement within and outside Australia will be associated with more cases. This was seen in Europe and Israel, when more movement of people occurred early in the northern summer. As there is near zero natural immunity to COVID in Australia, border controls and quarantine of those infected will continue, although screening of asymptomatic subjects may well be stopped. Given current “normalised” New South Wales numbers of 1200 per 10 million are stressing health systems (although low compared with six times that number recorded in “opened UK”), strategies to complement vaccine protection are urgently needed.
Waning post-vaccine immunity will exacerbate infection numbers and virus transmission in early 2022. As the pandemic evolves, the virus likely will adapt to its niche in the community, with a loss of its destructive power. The future use of vaccines is discussed below, but current experimentation with “booster” shots has little appeal on efficacy or safety grounds.
As borders are relaxed and international travel is resumed, the only logical and science-based way to reinforce vaccine protection is to adopt widespread use of re-positioned drug therapy.
THE roadmap for “escape”, as modelled by the Doherty Institute, anticipates transition to Phase B in late 2021 with minimal serious disease and hospitalisation requiring light social restrictions. Phase C is a consolidation period, prior to Phase D, when border restrictions are modified during the first half of 2022. Although this modelling was based on the Delta strain, it was released before the July-August third wave swept into Australia. The government strategy of accelerated vaccination and enforced lockdowns until achieving 80 per cent vaccination is already a rocky one.
Five months after receiving the Pfizer vaccine, protection in Israel against mild-to-moderate disease was only 15 per cent. The unpredictable nature of new variants leads to an increasing realisation that a COVID-free community in Australia will not happen without draconian and continued lockdowns. There is an immediate need for early drug therapy to complement the vaccine program.
Here is a summary of available drugs. This topic has been reviewed (see my contributions to Quadrant in January and June: and Phillip Altman’s in June), but it remains embroiled in misinformation, ideology, politics, and the commercial interests of Big Pharma. The imperative of a pandemic has focused interest on known drugs with excellent safety profiles.
These repurposed drugs come in two groups: drugs synthesised to have specific antiviral activity, and drugs that have less specific antiviral effect and that work through their capacity to disengage cell processes required for viral production. The first group are usually acquired by the pharmaceutical industry from academic institutions, then patented and sold at high cost. The second group of drugs have a biological origin with a history of many years as treatment for infectious and inflammatory diseases. They are no longer under patent.
Specific antiviral drugs have a lacklustre history as nucleic acid analogues used against RNA viral diseases such as influenza and Ebola. They block the RNA-dependent polymerase enzyme responsible for viral replication and incorporated into the viral RNA, rendering it ineffective. The best studied is Remdesivir, hailed as the “breakthrough” drug by Dr Tony Fauci, the leading American voice in COVID management. It was shown to reduce hospitalisation by only four days. Promoted by the pharmaceutical industry, this drug became standard treatment for hospitalised COVID patients despite randomised controlled trials (RCTs) failing to confirm benefit. Its use comes with concerning side effects and a cost of $4000 per course. Remdesivir was followed by two oral antivirals—Favipiravir, widely used with some success and costing $200 per course (its patent expired in 2020). More recently Molnupiravir has been developed, originally for influenza and Ebola. The pharmaceutical company Merck has initiated a “rolling registration” process with regulatory authorities across the world despite little evidence of efficacy and an emerging view that the RNA polymerase is a poor therapeutic target. Remarkably, the US government has bought the drug for A$1000 per course before trials are completed and efficacy proven.
The second group of re-positioned drugs has a long record of clinical use in a range of infections and chronic inflammatory diseases. The extensive history and width of benefit compared to the specificity of nucleoside inhibitors of RNA polymerase fuels a perception of irrelevance to COVID-19.
The best-credited drug is ivermectin (IVM). In brief, over sixty studies with 26,500 patients have been subjected to meta-analyses. These analyses identified significant benefit for IVM used as a prophylactic (86 per cent), early treatment (72 per cent), as well as reduced viral transmission. These figures are little changed when analysis was restricted to 31 RCTs. A meta-analysis of six quality peer-reviewed meta-analyses found a 58 per cent reduction of death. Regions in India, Mexico and South America, adopting widespread use of IVM, showed dramatic differences in case numbers and mortality compared to adjoining regions not using IVM.
Many studies, performed in the intensity of a pandemic, can easily be criticised by “experts” unfamiliar with clinical medicine. The consistency of data across many such trials involving great numbers of subjects and many non-aligned investigators led to three peer-reviewed sophisticated meta-analyses that “point overwhelmingly to the efficacy of IVM in both the prevention and management of COVID-19” (Kory et al J. Therapeutics 28(2021) e299-e318 DOI).
A formal review by Bryant and colleagues of 24 RCTs found “moderate certainty” evidence in support of IVM therapy. This is considered “more than sufficient for regulatory approval of existing drugs in a new indication”.
These quotes are included in a critique of the National COVID Clinical Evidence Taskforce (NCCET) statement on IVM by the epidemiologist Dr Tess Lawrie, based in the UK.
In her comprehensive rebuttal Lawrie identifies an out-of-date, cherry-picked overview that includes inaccurate, illogical and misleading comment, and the exclusion of significant data bases. She says the NCCET statement is “an agenda driven independently of the actual evidence”.
The importance of this evidence-based independent critique of the NCCET statement on IVM is critical, as professional bodies such as the Australian Medical Association and the Pharmaceutical Society of Australia, public authorities such as the Therapeutic Goods Administration, as well as the press and politicians, accept these views, and base actions on them without themselves examining the evidence. This accepting approach comes at a cost to infected patients and confuses doctors charged with treating them.
“AFTER the bubble” is the black-box period that follows the point of “bubble departure”. Yet it is of great importance for us to understand how COVID may affect our community in the longer term, given the profound implications as to how we would manage at personal and national levels. While predictions can be horribly wrong, in many ways COVID has followed a course that reflects the biology of airways infection. It carries added pathogenicity due to an extension of receptors into the gas exchange apparatus, bringing systemic immunity more into play, and the toxicity of the spike protein.
The current “third wave” caused by the Delta strain may be a transition zone to long-term seasonal COVID similar to the pattern for influenza following the 1919 pandemic. The Spanish flu infected at least 500 million with a 10 per cent mortality in three main waves over two years. This is twice the number infected with Covid, and ten times Covid’s mortality. Yet within a year, the pattern of influenza infections had returned to pre-pandemic seasonal influenza levels with a reported rate of about 0.1 per cent and a slight increase in mortality that lingered for fifteen years. There was no influenza vaccine until the late 1940s. Variants, due to antigen drift, maintained viral vigour, short of epidemic disease, until a major antigen change (or “shift”) in 1957, when seventy deaths were reported in Australia.
Population immunity was a critical determinant of this benign course. While the potential lethal possibilities of COVID cannot be forgotten, the Delta variant currently has the mortality of a bad influenza season. Current data from Sweden, with its high level of natural immunity, supports the idea that COVID infections in that country are approaching “normal” for influenza. The problem facing Australia is that with its Covid-free management policy, the population is immune-naive, and may struggle making the transition to the “new normal”.
WE know from Israeli data that current genetic vaccines do not protect against infection after six months and that their main value is to protect against severe disease. Similar data is emerging from the US, with retention of protection against severe disease, and with hospitalisation thirty times less among those vaccinated. Antibody levels following vaccination fall faster than those in convalescent sera. Immune memory and T-cell immunity persists and a combination of vaccination and infection maintains population immunity.
The current experimental genetic vaccines were introduced purportedly due to the need for speed to develop vaccines in a crisis. They are a basis for “escaping the bubble”, but are not a long-term answer. They produce uncontrolled amounts of spike protein which appear to be linked to a range of adverse effects including death. The reported mortality rates, in excess of thirty per million vaccinations across agencies in the northern hemisphere, is unacceptable in the longer term. For context, the highest reported number of deaths linked to an influenza vaccine was one per million, which led to its withdrawal. Current reports to VAERS (the US government reporting agency) of post COVID-vaccine deaths at 13,000 (or 65 per million vaccinated) is a concerning signal of toxicity. Adverse events are known to be under-reported and can be coincidental to the vaccine. Deaths temporally associated with COVID vaccines have been analysed by “rules of causation” and post-mortem studies concluding that vaccination may contribute to death in between 40 and 80 per cent of reports. Mechanisms appear to involve immune-mediated damage of host cells expressing spike protein. Subsequent vaccination or natural infection could initiate serious inflammation.
That genetic vaccines are in unknown territory is reflected in warnings from scientists, including Nobel laureate Luc Montagnier, identifying possible long-term outcomes that need study. They point to antibody-enhanced infection and emergence of variant viruses that could promote disease. Pathological outcomes raised include prion disease (including Parkinson’s disease and dementia caused by “prion sequences” within the spike protein), autoimmune disease (due to disturbed immune regulation and spike protein acting as an antigen), vascular disease due to spike protein toxicity to endothelium, and incorporation into host DNA using the cells’ reverse transcriptase capacity. Recent reviews that emphasise the importance of mutagenicity and transformation studies to screen for carcinogenicity are a reminder that Frank Graham, 40 years ago, in Canada, showed adenovirus vectors caused “transformation” in human cells.
There is simply insufficient data for long-term decisions. Basic cell research and vaccinology follow separate paths. Before long-term commitment to genetic vaccines, there is an urgent need for vaccine research to come together with mainline cell biology to give confidence on safety. Discussion of manufacturing genetic vaccines in Australia should not progress unless and until these questions are answered.
Vaccination for children is a hot topic. Analysis of COVID in those under 12 indicates that little benefit follows vaccination as children rarely get significant disease, “long Covid” is uncommon, and they are poor transmitters of infection. Vaccination will have little benefit, either for the child or the community. Vaccination for those aged between 12 and 18 is more difficult to assess, as few get significant illness, and adverse events increase. Resultant myocarditis is concentrated in young males, with figures peaking at 160 per million doses in those aged 18 to 24. Vaccination of those aged between 12 and 18 is an individual decision, with no clear evidence of any overall advantage.
It is clear that the biology of COVID-19 infection frames the space in which vaccines can work, and that genetic vaccines are no more effective than classic “antigen vaccines” — with the effective and (to date) safe NovaVax antigen vaccine to be available in Australia later this year. Every effort to develop antigen vaccines using non-spike protein as antigen, must be a goal for long-term vaccine development. Australia should take control of its COVID vaccine production, as it has with influenza.
AUSTRALIA’s path to escaping its COVID bubble will not be infection-free, as demonstrated by the current outbreaks. Vaccination rates at 80 per cent will be hard to achieve, as vigorous campaigns in countries more afflicted by COVID struggle to reach 70 per cent. At 70 to 80 per cent vaccination, Australia must expect infection rates greater than current ones, given the example of other Western countries as they resume “normal” international relationships. Iceland provides a model for Australia, with its maritime border. Its infection rate is a multiple of Australia’s current rate, so despite essentially no deaths it is putting extreme pressure on its medical facilities. Despite a vaccination rate now over 80 per cent, quarantine measures are again discussed, to the point of lockdowns, to protect health services. This is a warning to Australia that it should adopt wide usage of early drug therapy to complement vaccination to navigate its way out of its bubble.
The biology of COVID infection determines the space for vaccines. It is not surprising to find that the current vaccines fail to protect against infection (while still preventing serious disease) after about six months. The future for the current genetic vaccines must take into account concerning signals of severe adverse events including deaths, reported across the northern hemisphere, due to uncontrolled spike protein synthesis.
What is clear, yet resisted by authorities on flawed grounds, is the immediate need for effective and safe drugs for early treatment. Ivermectin, the lead candidate, would facilitate transition out of the bubble, reduce community transmission, serious disease and hospitalisation, and limit the need for any return to lockdowns.
The physician’s mantra remains, “There is no alternative treatment, patients get sick and die, the evidence is persuasive, what is there to lose?”
In the longer term, the hoped-for transition is to a situation similar to that of post-Spanish-flu in 1920, characterised by mild-to-moderate seasonal infections, beginning one or two years after the pandemic. The Delta variant may represent a transition phase, as appears likely in Sweden. Australia with its immune naivety may take longer to achieve such an outcome, requiring drug therapy and vaccines to cover the interim period. Mutant variants of COVID remain the unknown, although increasing population immunity should limit the severity of disease in most subjects, as it does with influenza. Seasonal antigen-based vaccines are likely to be paired with influenza vaccines for an annual “shot”, with both including antigens matched to the circulating species.
From a biological viewpoint, clinical outcomes of COVID infection are the balance of the host-parasite (virus) relationship. Over time, as the host acquires immunity and the virus adapts, clinical disease evolves from “the dramatic to the mild”, as did influenza in 1919 and 1920. Sweden appears to be close to achieving this with COVID. Will Australia’s focus on maintaining a COVID-free environment paradoxically delay this transition in Australia?
Professor Clancy is a practising clinical immunologist. He was Foundation Professor of Pathology at the University of Newcastle, where he established the Newcastle Mucosal Immunology Group, identifying mechanisms of airways protection and the pathogenesis of mucosal disease, and discovered new methods of disease control. He contributed the article “COVID-19: Where Are We At and Where Are We Going?” in the July-August issue
A Sad and Shameful Day for Australian Medicine
Professor Borody Talks about Early Treatment of COVID-19 – Part 1 – September 2020
Professor Borody Talks about Early Treatment of COVID-19 – Part 2 – September 2020
Letter to Australian Government’s Department of Health to recommend ivermectin
Australia’s TGA Bans GPs from Prescribing Ivermectin
Ivermectin. It’s as Aussie as Vegemite. The path out of the pandemic is under our noses.
‘It’s crystal clear’: Professor Robert Clancy backs ivermectin as a COVID-19 treatment