

Source: Rounding The Earth Author: Mathew Crawford
I’m sure this seems like a strange question for nearly everyone. After all, if that is the case, either the solutions require highly clever thinking, our public health officials are completely incompetent, or else officials are perfectly okay with passive statistical murder of millions of people.
And a lot of priors should be re-examined given the recent Fauci email dump, which is not simple to think through no matter how anyone frames it.
Or is there another explanation that I missed in my first paragraph?
Perhaps so, but I’m going to move forward with an argument that SARS-CoV-2 is far easier to handle than its public image suggests.
1. The virus is highly aerosolized and dies quickly to UV light and even ordinary light.
Remember that 99.9% or more of infections occur indoors (some of the 0.1% in that study were actually indoors, but in “outdoor settings”). Certainly the sunlight kills the virus quickly, but even at night the aerosol clouds likely float up, down, or away depending on the physics per virion particle size.
Some people worry about UV light being harmful to eyes and skin, of course. But there are wavelengths that kill the virus and are safe for human exposure. Sure, fitting UV lights in offices, public buildings, nursing homes, and classrooms would cost a pretty penny. But that several billion dollars would pale in comparison to the trillions spent on the pandemic while making Americans safe from all viruses.
Friends of mine fitted their central vacuum systems with UV cleansing. Somebody should do a study on transmission differentials between households and buildings with such systems installed (maybe they have, but I haven’t come across it).
Troubling Questions and Thoughts:
- Why did it take over a year for a lot of public health officials to state that the virus was aerosolized to such an extremely fine level?
- Is there a reason that public health officials want for Americans to actually catch a lot of viruses, like building general herd immunity for the lot of them?
- Is the moral hazard of the immense profit motive enough to squelch any conversation of such a solution?
- Nations in Asia and Africa with low rates of infection include some areas where window are often left open, or are non-existent. What if…just leaving more windows open or staying outside in the gloriously cleansing sunshine is enough to end most of the pandemic (outside of harsh winter weather moments, of course)?
2. We Have Antiviral Agents.
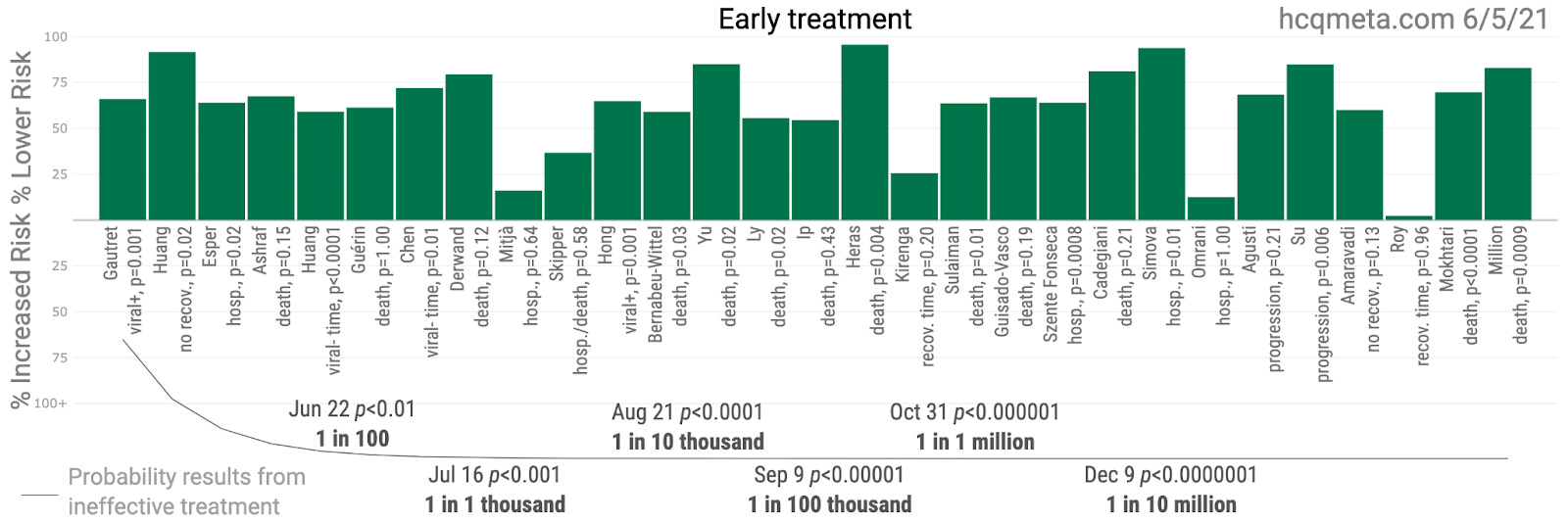
While historically speaking, there are few good antiviral medications leading to an outdated set of priors among many researchers and physicians, that fact began to change as quinine (also here and here) and then its derivative hydroxychloroquine demonstrated antiviral activity (also here, here, here, here, and here across many families of viruses). And there is good rationale for repurposing of these drugs since these antiparasitics work along the same receptor pathways through which SARS-CoV-2 and some other viruses infect humans. The best results of HCQ studies in treating COVID-19 come from the “early treatment” category, which is indicative of antiviral action.
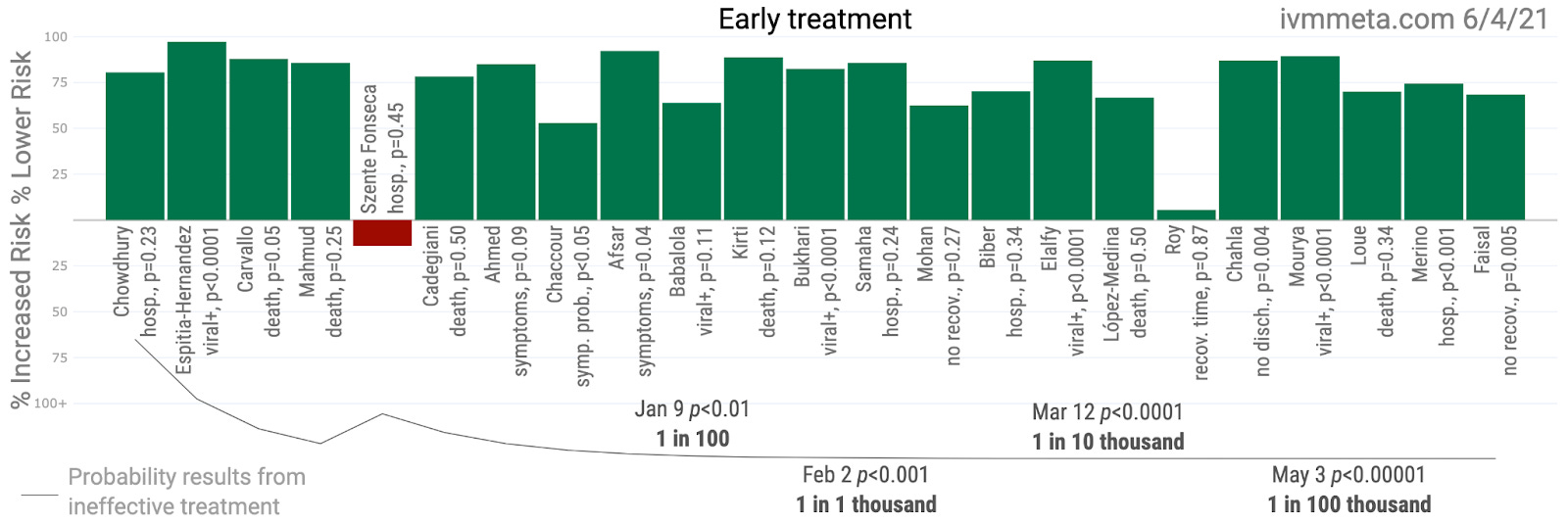
Similarly, the antiparasitic ivermectin previously showed promise as an antiviral for partially similar and partially different reasons (here, here, and here where ivermectin is called a “wonder drug” in 2017). Here is the summary of ivermectin’s early treatment research to date:
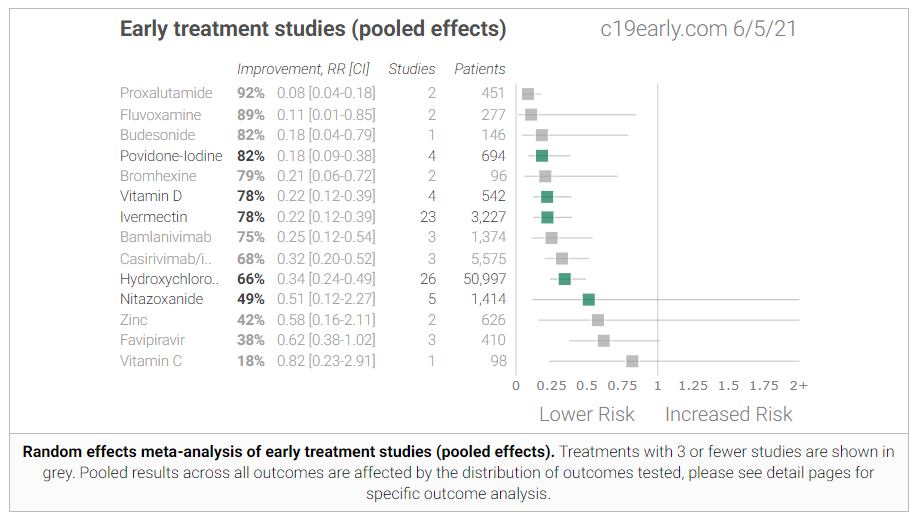
It turns out that a whole bunch of drugs show early efficacy, indicating that there may be a whole lot of effective antivirals in combating SARS-CoV-2! While this may seem counterintuitive, these results may indicate a relationship between the tiny virion size in which small viral loads of the novel coronavirus are transmitted at a time, possibly (probably) making the job of each antiviral agent a little easier.
Troubling Questions and Thoughts:
- Why is nobody in public health talking about the pandemic in these terms? To whom is it not obvious that the best time to apply an antiviral agent is early during the viral replication process?
- Why is nobody in government investigating the meaning or perpetrators of the numerous studies against HCQ that appear fraudulent or rigged on face?
- Why do authorities such as the WHO prefer to test HCQ and other agents as late treatments, after viral replication has stopped?!
3. People seem to gain substantial protection from SARS-CoV-2 and COVID-19 from numerous vitamins and minerals.
These include
- Zinc: 10 studies with great overall results and a 2010 paper showing that zinc inhibits coronavirus and arterivirus RNA polymerase activity in vitro
- Vitamin C: 10 studies with great overall results.
- Vitamin D: 80 studies with largely positive results, and numerous prior studies showing potentiality of vitamin D as an antiviral agent (here and here and especially here). Heck, Vitamin D maintenance should be a global health priority.
- Folic Acid: There is mechanistic speculation that folate helps that apparently still hasn’t been peer reviewed and published after nearly 15 months?! There are also hospital reports in the UK that show that pregnant women get hospitalized at far lower rates (also in Mexico) for COVID-19, particularly during the period when they would be supplementing with folate. While the evidence is certainly not conclusive, it is consistent with evidence that folate helps pregnant women avoid influenza.
- Others: There is at least some evidence for niacin, iron chelation therapy, magnesium, B12, and selenium. I haven’t read all of it to know how well I trust it, but I see various doctors promoting some of these.
While I wouldn’t say, “just take your vitamins and that’s all we need until herd immunity,” there are researchers who prefer that strategy to vaccination. I just happen to think we have a lot more options. The fact of the matter is that vitamins and minerals have long been given light lip-service, but still overlooked in the prevention and treatment of viral or respiratory infections in particular.
Troubling Questions and Thoughts:
- Might medical authorities be generally interested in letting more people get sick in order to further study illness for any reasons, including possibly gathering data to understand biowarfare? Given the window we’re seeing into gain-of-function research and its motivations, we should not be entirely shocked at any answer.
- Is there any reason at all to tell people to “sit at home and do nothing and wait to see if you get sicker” rather than “take your vitamins and minerals and maybe get OHD25 (hormonal vitamin D) levels checked by a doctor if you have more than the lightest of symptoms or might be in a high risk group”? How can this possibly make any sense at all? Even if over one hundred mostly positive research papers turned out to be random noise by pure coincidence, the cost is extraordinarily low.
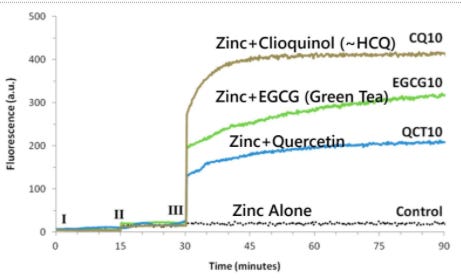
4. Zinc Ionophores deserve a lot more attention.
Each of chloroquine, hydroxychloroquine, quercetin, teas (green teas in particular), PGG, EGCG and many of the local remedies used in China and other nations are zinc ionophores with varying levels of studied efficacy. Such efficacy is likely understated in the research, but the correlation of results across this agent class is highly suggestive of mechanistic causation.
5. Oral and Nasal Sprays Show Dramatic Efficacy.
As with antivirals, these agent+delivery combinations may do specifically better against SARS-CoV-2 due to the small virions in aerosol clouds of virus.
Copy-pasted straight from my notes, this is only a partial list of those I’ve seen, but understand that my time is limited and I have over a thousand pages of notes that are largely this concise:
- Mar 26, 2021 (Ferrer and Gonzalez) Effective Nasal Disinfectants Overlooked Strategy
- March, 2021 (nocamels) SaNOtize begins production of anti-COVID nasal spray in Israel
- Apr 12, 2021 (the-sun) Nasal spray kills 99.99% of CoV (SaNOtize again)
- Apr 20, 2021 (Seet et al) Oral HCQ and povidone-iodine throat spray; vitamin C placebo
6. Even Remdesivir seems to work, a little, and might be sometimes worth gambling on renal failure if you’re trapped in a hell of no other options.
While proponents of the most well-studied early treatment agents such as HCQ and ivermectin love to dunk on remdesivir, while is absurdly expensive and netted Gilead a few billion dollars in revenue during the pandemic, the overall body research indicates that remdesivir likely has a small positive effect. Part of what is interesting about this is that remdesivir has never been tested as an early treatment medication! The rationale for using remdesivir was that it showed in vitro antiviral action against SARS-CoV-2. But it’s just too expensive to use on so many patients early on, prior to moderate or severe COVID-19.
Troubling Questions and Thoughts:
- The evidence of remdesivir’s efficacy has never been nearly as strong as that for HCQ, but it may have been easier to let this medicine proliferate as a treatment before reining it in in order to pave the way for the many-billion-dollar vaccine campaign. Not being used as early treatment, it did not open the door to the general question about early treatment medications.
- Almost nobody even realizes that remdesivir is an antiviral, meaning almost nobody would ask the right questions about this piece of the Big Picture.
7. All the Other Stuff
Antibiotics, corticosteroids, monoclonal antibodies, interferon treatment, plasma therapy, and even erectile dysfunction drugs if you’re feeling adventurous! The virus or the disease state can both be attacked from many angles. Even antidepressants have shown promise.
I’m sure I missed a few! Feel free to leave them in the comments and please include links.
8. Ring Strategies Can Protect High Risk Targets
There are so many ways to attack this virus, and for the remaining targets, there is a tried and true strategy of protecting just them, whether with vaccinations or other strategies. Sweden went this route even without using most of the treatments above and their “rank” in the deaths/million list has been steadily falling for more than a year now.
Troubling Questions:
Where are the adults in the room?
What the hell are we doing?
What is the endgame of pretending like we’re not living through an avalanche of deadly lies?
The Chloroquine Wars Part X – A Discussion of the Insanity of the Chloroquine Wars
The Chloroquine Wars Part XI – See No Good, Hear No Good, Speak No Good
The Chloroquine Wars Part XII – Manufactured Fear During Hydroxychloroquine’s Trump Moment
The Chloroquine Wars Part XIII -A Clockwork Orange Man
The Chloroquine Wars Part XIV – How to Rig Research: Surgisphere Part I
The Chloroquine Wars Part XVII – Why the Story About India’s April COVID-19 Spike is All Wrong
The Chloroquine Wars Part XV – How to Rig Research: Surgisphere Part II
The Chloroquine Wars Part XIX – Historical Failures of Public Health Authorities
The Chloroquine Wars Part XX – Why The Early Treatment Data is Better Than Anyone Imagines
Doctor Didier Raoult Part I: Where We Are Now -The Chloroquine Wars Part XXV